Junctional Beats During Cryo-Ablation Of The Slow Pathway For The Elimination Of Atrioventricular Nodal Reentrant Tachycardia
Murat Sucu, Vedat Davutoglu, Esra Polat
Gaziantep University Medical Faculty Department of Cardiology Gaziantep Turkey.
The patient was a 39-year-old female with recurrent paroxysmal, regular narrow QRS complex tachycardia. Atrioventricular nodal reentrant tachycardia (AVNRT) was induced. The cryo-ablation attempts (-80°C, 240 second) were performed in the inferior–posterior triangle of Koch. We observed several junctional beats during cryo-ablation. After successful cryo-ablation, AVNRT induction was repeatedly checked during a waiting period of 30 minutes without recurrence. In our case we demonstrated that junctional beats can be observed during cryo-ablation. We believe this to be the first description of junctional beats occurring during cryo-ablation of AVNRT.
Key Words : AVNRT, Cryoablation, Junctional Beat.
Correspondence to: Murat Sucu, Gaziantep University Medical Faculty Department of Cardiology Gaziantep Turkey.
The patient was a 39-year-old female with recurrent paroxysmal, regular narrow QRS complex tachycardia. The patient had signed informed consent before the baseline electrophysiology study and patient was investigated in the fasting state without sedation. All anti-arrhythmic drugs were discontinued for at least five half-life periods. Surface electrocardiography (ECG) and endocardial electrocardiograms were recorded on a multichannel recording system (Pruka Cardiolab, GE HealthCare, Milwaukee, WI, USA). Two 6 F diagnostic quadripolar catheters were inserted percutaneously via the right femoral vein and positioned in the high right atrium, His-bundle region. A 6 F decapolar catheter was inserted via right femoral vein and placed inside the coronary sinus. A standard electrophysiology study was performed. Baseline surface electrocardiogram was normal and intracardiac intervals revealed an HV interval of 44 ms after programmed atrial stimulus. The tachycardia cycle length was 260 ms, and earliest retrograde atrial activation at the His bundle catheter. AVNRT was induced and diagnosed on the basis of standard diagnostic criteria. Dual AV nodal physiology was determined by a sudden AH or HA jump of at least 50 ms in response to programmed atrial or ventricular extra stimulation or demonstration of dual AV node physiology with earliest retrograde atrial activation at the His bundle catheter, measured ventricular atrial (VA) time<70 milliseconds during tachycardia. A combination of intracardiac electrocardiograms and anatomical approaches was conducted to identify target sites for ablation of the slow pathway in the triangle of Koch. Cryo-ablation was performed using a 7 Fr cryocatheter (Freezor® Xtra, CryoCath Technologies, Quebec, Canada) with a 6 mm-tip electrode. Cryo-mapping was carried out first at a temperature of -30°C for a maximal duration of 30 seconds to test the electrophysiological effect on the target sites using programmed stimulation that reproducibly demonstrated dual nodal physiology or induced AVNRT.
Four corresponding cryo-ablation attempts (-80°C, 240 seconds) were performed in the inferior–posterior triangle of Koch. If AVNRT was still inducible, cryo-ablation was interrupted and cryo-mapping was performed at the new target sites. We observed several junctional beats during each attempt at cryo-ablation, cryo-ablation, and immediately we stopped cryo-ablation application (Figure 1). When junctional beats occurred during cryo-ablation, the catheter was moved more posteriorly, resulting in successful ablation without complication. After successful cryo-ablation, AVNRT induction was repeatedly checked during a waiting period of 30 minutes.
Radiofrequency (RF) ablation of the slow pathway has become first-line therapy for the treatment of AVNRT. Cryo-ablation provides a useful, safe technique for slow pathway ablation. The ability of cryo-ablation to test the functionality of specific ablation sites before production of a permanent lesion may eliminate accidental AV block.1 During cryo-ablation, usually accelerated junctional tachycardia is not seen and therefore cannot guide lesion delivery.
In every attempt within 80-100 second of cryo-ablation we observed junctional beats in all four cryo-ablations but we did not see junctional beats during cryo-mapping. When junctional beats occurred during cryo-ablation we terminated and the catheter was moved more posteriorly. As it is well known that during cryoablation catheter movement is difficult since the catheter is freezing, the junctional beats can not be attributed to the mechanical effect of catheter movement. Taken together, in our view, the junctional beats in our case likely did not stem from mechanical effect of the His catheter.
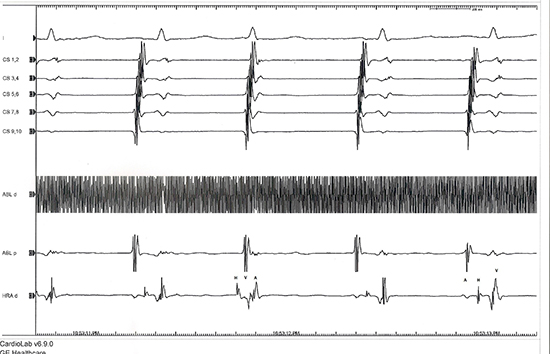
Figure 1: The panel is arranged from top to bottom as leads D1, coronary sinus (CS 9,10 proximal, CS 1,2 distal) and ablation catheter (Abl) in the triangle of Koch’s high right atrium (HRA) catheter in the His bundle area. A junctional beat on cryo-ablation (the third beat). (A: atrial electrogram, V: ventricular electrogram, H: His electrogram)
We believe this is the first report of junctional beats occurring during cryo-ablation of AVNRT. The accelerated junctional tachycardia was seen on re-warming in during cryo-ablation.1,2 Nguyen et al. reported transient accelerated junctional rhythm late after para-Hisian accessory pathway cryo-ablation.2 Recently, Drago et al. have reported in the post ablative period, junctional arrhythmias occurred in 2 patients, and they claimed that probably it was due to a direct trauma or inflammatory reaction very close to the compact AV node.2 In our case we demonstrated that junctional beats can be observed during cryo-ablation. The implication and pathophysiologic mechanism of this event need to be clarified in further studies.






