The A That Did Not Fib:Two Roads Both
Traveled By
James C. Hansen, MD, Abraham G. Kocheril, MD, FACC, FACP
University of Illinois at Chicago,Chicago, IL 60612, USA.
A 64-year-old woman presented with palpitations. Her 24-hour Holter monitor revealed runs of presumed atrial fibrillation (AF). The patient was referred for EP study and AF ablation.
At EPS, an anterograde A-H jump was noted. Spontaneous bursts of tachycardia were seen, consisting of sinus atrial beats with dual ventricular responses, each preceded by a His deflection. There was no atrial fibrillation during the study. Radiofrequency ablation of the slow AV node pathway was performed. There were no inducible tachycardias and no A-H jump following the ablation. The patient had no recurrence post-procedure.
This case presents a rare example of simultaneous dual anterograde AV-nodal conduction. The conditions leading to this phenomenon include dual AVN pathways, markedly slowed conduction in the slow pathway, and lack of retrograde conduction up either pathway such that reentry was impossible. An irregular, narrow-complex tachycardia resulted, initially interpreted as AF. Slow-pathway ablation was curative.
Correspondence to: James C. Hansen,Section of Cardiology(MC 715),840 South Wood Street,Chicago, IL 60612, USA.
Catheter ablation of atrial fibrillation (AF) has become an increasingly prominent treatment option for patients refractory to antiarrhythmic therapy. As the population of patients referred for AF ablation has grown, so necessarily has the number of invasive assessments of narrow-complex tachycardias. We present a patient referred for AF ablation who was found instead to have a rare tachycardia due to sinus rhythm with simultaneous dual anterograde atrioventricular node (AVN) conduction.
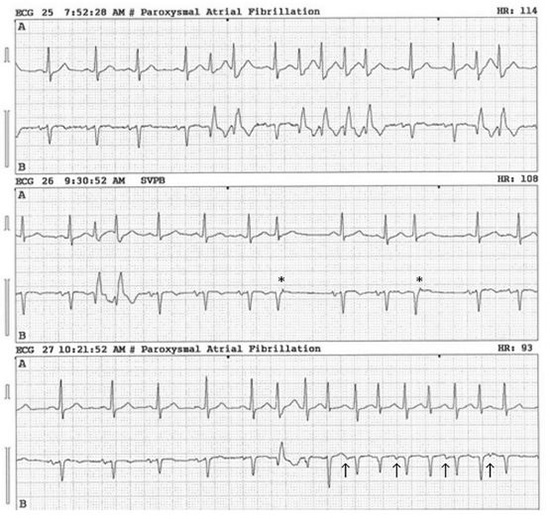
A 64-year-old woman with a history of hypertension and systemic lupus erythematosus presented with several months of intermittent palpitations. Physical exam and electrolytes were unremarkable, and echocardiography revealed normal left ventricular systolic function. A 24-hour Holter monitor revealed frequent premature atrial contractions (PAC’s) with right bundle branch block (RBBB) aberrancy, correlated with symptoms of palpitations. There were also runs of presumed atrial fibrillation (AF), for which the patient was started on warfarin (Fig. 1). Given her frequent, distressing symptoms and lack of response to medical therapy, she was eventually referred for electrophysiology study (EPS) and possible ablation of AF.
Figure 1. Representative consecutive telemetry strips from 24-hour Holter monitoring. Paroxysms of irregular tachycardia, occasionally with RBBB aberration, are noted. Asterisks ( * ) indicate likely retrograde p-waves. Arrows ( ) denote sinus p-waves. Initial interpretations are noted at the top of each strip (SVPB: Supraventricular Premature Beat)
At EPS, an anterograde A-H jump was noted, suggestive of dual AVN physiology (Fig. 2). No V-A conduction or echo beats were seen. There were spontaneous bursts of tachycardia, consisting of sinus atrial beats with dual ventricular responses, each preceded by a His deflection (Fig. 3). The H-V interval was stable at 57 msec, and ventricular refractory period (VERP) was 230 msec. There was no evidence of atrial fibrillation during the study. RBBB aberrancy was noted with PAC, rapid atrial pacing, and with simultaneous dual-pathway complexes. No additional arrhythmias were induced with IV isoproterenol. Radiofrequency ablation of the slow AVN pathway was then performed. There were no inducible tachycardias and no A-H jump following the ablation. The patient tolerated the procedure well, and was discharged home the next day. She had no recurrent symptoms during several months of follow-up.
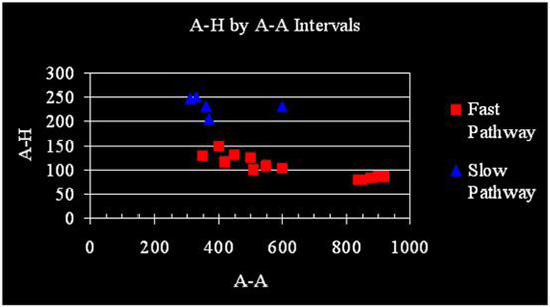
Figure 2. Anterograde A-H Jump. A-H intervals are plotted against preceding A-A intervals. Two populations of responses are seen. The blue triangles indicate likely slow-pathway responses and red squares denote fast-pathway conduction. Slow-pathway conduction predominates below A-A of 370 msec, the refractory period of the fast pathway. Note the rare slow pathway response at the longer cycle length of 600 msec. The slow responses seen likely represent a degree of concealed conduction from slow pathway into fast. Not depicted are the very slow A-H encountered only with dual anterograde responses (see text)
This case presents a rare example of dual simultaneous anterograde AVN conduction causing symptomatic non-reentrant tachycardia, with successful radiofrequency ablation of the slow pathway leading to resolution of the tachycardia and symptoms. Dr. Kenneth Rosen and colleagues at the University of Illinois at Chicago first reported dual-AVN physiology in patients with paroxysmal supraventricular tachycardia (SVT) in 1973.1 The common clinical pathophysiology arising from dual AVN conduction is atrioventricular nodal reentrant tachycardia (AVNRT), for which definitive treatment is catheter ablation of the slow pathway or pathways.
In this case, the patient’s symptomatic SVT was the result of sinus beats with anterograde conduction down both AVN pathways without reentry, leading to tachycardia via ventricular rates double the sinus rate. Conditions necessary for this phenomenon include dual AVN physiology, markedly slowed conduction in the slow pathway (A-H2 exceeding A-V1 + VERP), and lack of retrograde conduction up either pathway, such that reentry is not possible. While dual responses can also be seen with accessory pathways, the H-V interval was stable in this case, and preexcitation was not suspected.
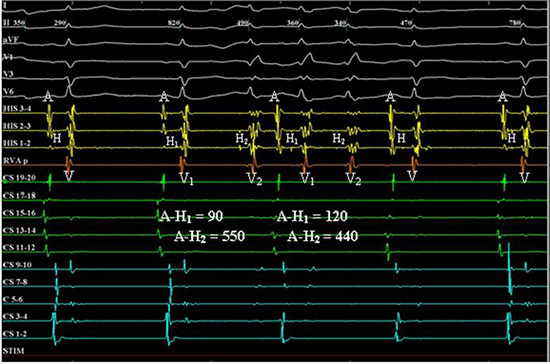
Figure 3. Dual Anterograde AVN Responses. Intracardiac electrograms are shown. Sinus atrial impulses (A) proceed at basic cycle length, with two consecutive instances of dual ventricular response (V) to a single A, followed by two singly conducted beats. Each V is preceded by a His recording. Note the marked variability of the A-H2 intervals leading to irregularity of the ventricular responses. Rate-related RBBB is seen. (I, II, aVF, V1, V3, V6: surface EKG. HIS: His-bundle recordings. RVAp: Right Ventricular apex. CS 11-20: Right atrium. CS 1-10: Coronary sinus. STIM: Pacing stimulus, inactive in present panel. Intervals listed are in msec)
Radiofrequency ablation of the slow pathway abrogated dual anterograde conduction and our patient’s symptoms, and no further tachycardia was inducible. Besides tachycardia from dual anterograde AVN conduction, other possible diagnoses include automatic junctional tachycardia (AJT), nodofascicular tachycardia, or AVNRT with proximal common pathway block.2 In AJT, inducibility with PAC would not be expected, and response to slow-pathway ablation is less likely. Nodofascicular tachycardia can present with an initial dual-AVN response, but is often preexcited and unresponsive to slow-pathway ablation. AVNRT with proximal block would be a regular tachycardia, and ventricular echo beats should be elicited. While our case had possible atrial echo beats on ambulatory monitoring (Fig. 1), no reentry was seen on EPS, and her tachycardia was irregular.
Slow-pathway conduction in our case exhibited marked variability in A-H interval (Fig. 3), leading to irregular ventricular responses interpreted as AF on the surface EKG. This likely represents concealed conduction between the fast and slow pathways. In particular, distal slow-pathway refractoriness concomitant with a refractory proximal fast pathway likely contributed to the slower population of responses at A1-A2 coupling intervals less than 300 msec shown in Fig. 2. Exclusive slow-pathway conduction without concealment into the fast pathway, giving A-H intervals in the 400-600 msec range, was only seen with H2-V2 beats in the setting of dual anterograde responses. The variable nature of the crosstalk between the fast and slow pathways reflects a complex interaction between the two pathways’ conduction properties, as influenced by autonomic tone and decremental conduction due to slight variations in the preceding A-A intervals. The complexity of these relationships may in part explain the lack of response to pharmacologic therapies seen in our patient and elsewhere, as a drug may alter conduction in fast pathway, slow pathway, and between the two, without alleviating the tachycardia or even worsening it by increasing the frequency of dual anterograde responses.
Tachycardia due to dual anterograde AVN conduction has been reported rarely since the first account of dual anterograde responses by Rosen in 1975.3 Sequelae of this condition have ranged from palpitations to tachycardia-induced cardiomyopathy.4-9 As in this case, patients can be misdiagnosed with atrial fibrillation due to irregularity in the responses.7,8 The tachycardia is also often resistant to or worsened by pharmacologic therapy, as it was with our patient. Treatment with ablation of the slow pathway is curative.6 This case demonstrates a rare consequence of dual AVN physiology and offers some insight into the nature of AVN pathways.






