Malignancy Associated Iatrogenic Iliopsoas Abscess -Venous Access Complication From Ablation Procedure
Sandia Iskandar MD, Moustapha Atoui MD, Muhammad Rizwan Afzal MD, Madhav Lavu MD, Madhu Reddy MD, Dhanunjaya Lakkireddy MD
Division of Cardiovascular Diseases, Cardiovascular Research Institute, University of Kansas Hospital & Medical Center, Kansas City, KS.
Iliopsoas abscess is a rare condition with a high rate of mortality and morbidity if left untreated. It can occur from hematogenous or lymphatic spread from distant structures or as a result of contiguous spread from adjacent structures. The disease typically occurs in patients with immunocompromised status and the symptoms can be non-specific.1,2 Generally, infectious complications from venous access during atrial fibrillation (AF) procedure are uncommon, and an iatrogenic iliopsoas abscess from percutaneous cardiac procedures has never been reported. We present the first case of iliopsoas abscess from an ablation procedure.
Key Words : Psoas Abscess, Ablation, Femoral Venous Access., Peripheral Vascular Disease.
Correspondence to: Dhanunjaya Lakkireddy,
Division of Cardiovascular Diseases, Cardiovascular Research Institute, University of Kansas Hospital and Medical Center, 3901 Rainbow Boulevard
Kansas City, Kansas 6616.
A 64-year-old Caucasian male with history of coronary artery disease, persistent AF, hypertension, and peripheral vascular disease was admitted for AF ablation. Surgical history includes aortobifemoral bypass and multiple hip arthroplasties due to trauma 15 years ago. He does not have a history of intravenous drug use (IVDU), inflammatory bowel disease (IBD), or any other immunocompromising conditions.
During the procedure, routine bilateral femoral and right internal jugular veins were used for intravenous access. After standard aseptic method, a modified seldinger technique was used for all venous access. A duo-decapolar deflectable catheter was advanced to the coronary sinus and the lateral right atrium through an 8-F short sheath in the right internal jugular vein. An 11- French (F) AcuNav “Siemens” catheter was advanced via the left femoral vein to guide the transseptal punctures. On the right femoral vein, a 3.5mm “Thermocool SmartTouch” ablation catheter and 20mm “Lasso” circular mapping catheter were advanced to the left atrium through 8.5-F and 8-F SL-1 sheaths, respectively. At the end, the catheters were removed and the long SL-1 sheath was exchanged for short sheaths. The sheaths were then removed and a manual pressure was performed until adequate hemostasis. During his stay, he did well without any complication or access issue. Standard groin care instructions were given.
Figure 1 Transverse section of the CT shows multiloculated fluid collection arising from the left iliac fossa measuring ~ 6.2 x 7.5 cm involving the involving the left psoas, iliacus, and quadratus lumborum muscles
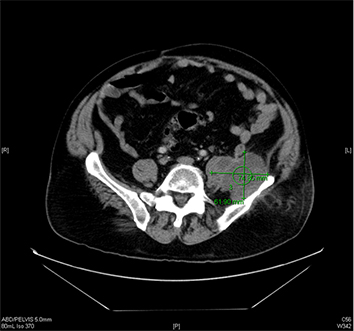
One week after the procedure, the patient developed left groin pain radiating to the left knee. The patient denied any fever, weight loss, night sweat, chills or rigors. A conservative management using NSAIDs was opted. The pain continued to worsen prompting an emergency room (ER) visit. On ER presentation, his vital signs were within normal limits. Physical examination was positive for pain on the left hip that was exacerbated by palpation. A 3 x 8 cm area of erythema and tenderness on the left flank was noted. The femoral vein area was thoroughly examined. The area was well healed without any sign of infection. Cardiovascular examination was negative for murmur. Laboratory examination revealed mild leukocytosis (WBC=14.5 K/uL). Other important pertinent laboratory tests include ESR (53 mm/hr), CRP (10.51 mg/dL), Creatinine (1.59 mg/dL), Lactate (1.3 mmol/L) and Creatine Kinase (46 U/L). Urinalysis was unremarkable. CT scan of the abdomen revealed an approximately 6 cm multiloculated fluid collection arising from the iliac involving the left psoas, iliacus, and quadratus lumborum muscles Figure 1 and 2. In addition, a curvilinear, soft tissue density mass in the central mesentery measuring 2.5 x 6.4 cm was also found. The vascular grafts from prior procedures were widely patent. CT guided abscess aspiration and drain placement were performed. Prior to the culture data, the patient was treated empirically with vancomycin and piperacillin/tazobactam. Microbiology examination revealed Eschericia coli and Prevotella loeschii. The flow cytometry did not reveal any malignancy. The patient was treated according to the culture and sensitivity data with ertapenem 1 gram daily from the time of drain removal for a total of two weeks. The patient remained stable and was discharged with a close follow-up. The patient was scheduled for biopsy of the suspicious mass in the central mesentery.
Two months after the ablation procedure, the patient was seen in electrophysiology clinic for follow-up. At that time, he had finished the antibiotic course and felt well. From a cardiac standpoint, he remained asymptomatic from his AF after the ablation procedure. Despite lack of symptoms, due to the significant size of the mesenteric mass, the patient underwent exploratory laparotomy and biopsy of the suspicious mass as planned. Pathology examination confirmed grade 1-2 (low grade) follicular lymphoma. The patient subsequently had PET scan for staging purpose. There was no other suspicious lesion identified and the retroperitoneal abscess previously drained a couple months earlier had improved, consistent with a positive response to antibiotics. The patient was referred to an oncologist for further treatment. Due to the indolent nature of this lymphoma, close follow-up with imaging was recommended; however, no treatment was necessary at this stage.
Iliopsoas abscess is rare and typically occurs in a high-risk population such as patients with diabetes, malignancy, HIV, IV drug users, and other immunocompromising conditions. It can be classified as primary or secondary. Primary psoas abscess typically involves hematogenous or lymphatic spread from a distant site.1,2 It is typically monomicrobial with Staphylococcus aureus as the most common organism.3 The rich blood supply of the iliopsoas muscles predisposes it to the primary infection.4 Secondary psoas abscess, on the other hand, occurs from contiguous spread from an adjacent infectious area.5 This is typically polymicrobial infection involving enteric bacteria from gastrointestinal tract, genitourinary tract, and vasculature.4
In this case, malignancy is one of the possible risk factors that likely contributed to the immunosuppressive state and predisposed him to develop iliopsoas abscess. As described in some case reports, malignancy can often mimic psoas abscess;6,8 however, these patients typically did not improve with antibiotics. On the other hand, colorectal malignancy, inflammatory, or any infectious process in the colorectal area, although uncommon, can cause micro-perforation with subsequent gut bacteria leakage causing abscess formation. However, in this case, there was no evidence to support this process as a mechanism; therefore, considering the timing of presentation post ablation procedure, we believe this was caused by vascular access contamination.
There were only two reported cases of iliopsoas abscess as a complication of vascular access. These involve central venous catheter (CVC) and dialysis catheter. Kwok et al. reported psoas abscess from subclavian central venous catheter.9 Similarly, Hsiao et al. reported iliopsoas abscess from tunneled jugular vein catheterization in a hemodialysis patient.10 On both of these cases, the catheter was placed >72 hours, whereas in our case, the access catheters were only placed for less than four hours.
Most venous access complications in electrophysiology procedures involve superficial skin and subcutaneous infections, hematoma, pseudoaneurysms, and arterio-venous fistula. Infectious complication from femoral arterial access during the cardiac catheterization procedure is estimated to be less than 0.1%.11 Femoral access complications are often associated with location of puncture, number of attempts, catheter material, and catheter size. Other possible causes include compromised technique, poor hygiene, prolonged indwelling sheath time, and the femoral access closure device.12-15
Possible sources of infection associated with CVC include colonization of the skin, intraluminal contamination, and rarely contamination of the infusion fluid.16 Biofilm depositions on the internal and external surface of vascular catheters play an important role in the colonization process.17 Intraluminal contamination typically occurs when the catheter is in place for more than two weeks or in patients with implanted devices.18 Contamination of infusion fluid generally involves gram-negative bacilli.16 Our case is unique in several ways: first, the access site was without any sign of infection, and most importantly, the catheter was only placed for a short period of time.
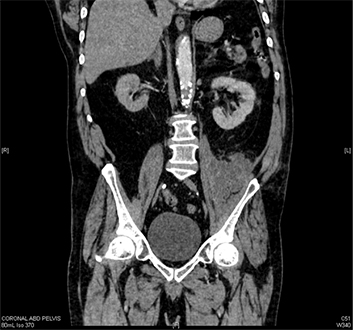
Figure 2 Coronal section of the abscess
It is unclear whether our case represents primary or secondary infection. Although the negative blood culture and the type of microorganism point towards secondary infection as a cause, the presence of infection foci and the subsequent contiguous spread were not evident. Besides malignancy, other possible reasons that could have predisposed this patient to this condition are the presence of a foreign body implantation such as a vascular graft and his history of multiple pelvic surgeries involving bone grafts, although these structures did not appear to be infected from the CT scan. In this case, perhaps his altered pelvic anatomy predisposed him to develop retroperitoneal infection.
This case report highlights the importance of careful vascular access preparation to prevent contamination and raise awareness that fatal vascular access complication can occur. Electrophysiologists should be aware of the risk factors associated with infection and should further evaluate patients, especially when pain develops late after the ablation procedure.
• Psoas abscess is rare and typically occurs in patients who are immunocompromised.
• Infectious complication from vascular access, associated with ablation procedure, is rare but can be fatal if not diagnosed early.
• The symptoms of psoas abscess are non-specific and highly variable; therefore, a high index of suspicion is needed.
• Altered pelvic anatomy and the presence of a foreign body from a medical device implantation may predispose patients to develop psoas abscess.
• Electrophysiologists should re-evaluate and perform detailed examinations in patients who complain of worsening groin or pelvic pain after the ablation procedure.






