Focal Atrial Fibrillation from the Superior Vena Cava
Andres Enriquez1, Jackson J Liang1, Pasquale Santangeli1, Francis E Marchlinski1, Michael P Riley1
1Section of Cardiac Electrophysiology, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania.
We report the case of a 66 year-old male who underwent catheter ablation for drug-refractory paroxysmal atrial fibrillation (AF) at our institution. Radiofrequency catheter ablation was performed using a three-dimensional electroanatomical mapping system. During ablation of the pulmonary veins (PV), right atrial ectopics were noted to repeatedly trigger AF and atrial tachycardia (AT). After PV isolation, mapping of the right atrium revealed that the superior vena cava (SVC) was in AF, while both atria were in an organized AT. Segmental ablation was performed around the SVC ostium, resulting in vein isolation and immediate restoration of sinus rhythm, while the SVC remained in AF. This case highlights the importance of the SVC in some AF patients as a potential source for non-PV triggers. SVC isolation can be safely achieved in most cases to improve outcomes.
Key Words : Atrial fibrillation, Superior vena cava, Nonpulmonary triggers, Catheter ablation.
Correspondence to: Dr. Michael Riley, MD Section of Cardiac Electrophysiology Hospital of the University of Pennsylvania 9 Founders Pavilion, 3400 Spruce Street, Philadelphia, Pennsylvania Email: Michael.Riley@uphs.upenn.edu. Fax: + 1-215-6624212 Tel: + 1-215-6624212
Pulmonary vein (PV) isolation is the most frequently used ablation strategy in patients with paroxysmal atrial fibrillation (AF). However, in a significant proportion of patients non-PV triggers may play a role in AF initiation, and several studies suggest that ablation of non-PV triggers, in addition to PV isolation, significantly improves long-term outcomes [1]-[4].
A 66 year-old male with a 3-year history of paroxysmal AF was referred for catheter ablation. His past medical history included hyperlipidemia and benign prostate hyperplasia. Previous transthoracic echocardiography revealed a normal left ventricular size and systolic function (LVEF 60-65%) with normal left atrial size (3.2 cm). He did well on Metoprolol and Digoxin until recent months, when he started experiencing more frequent episodes, especially with exercise.
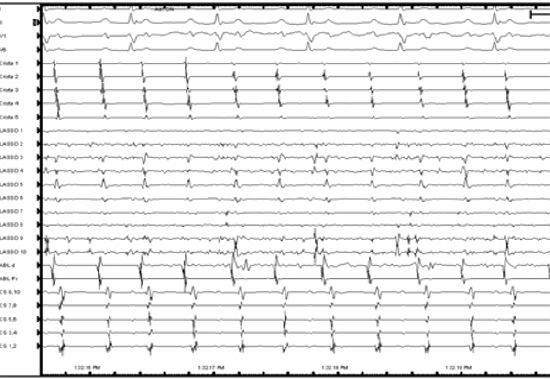
The patient presented to the electrophysiology laboratory in sinus rhythm. The procedure was conducted under general anesthesia and mapping and ablation was aided by EnSite NavX system (St. Jude Medical, Minneapolis, MN). During ablation of the PVs the patient went into AF, triggered by right atrial ectopics with earliest activation recorded at the distal crista catheter [Figure 1]. Eventually, the AF organized into a regular atrial tachycardia (AT) (CL 320 ms), also earliest at the distal crista, positioned at the superior vena cava (SVC)-right atrium (RA) junction. After completion of PV isolation, the catheters were withdrawn back into the RA and the Lasso catheter was advanced into the SVC. Interestingly, the SVC was found to be in AF, while both atria remained in AT [Figure 2].
Figure 1. AF initiation triggered by atrial premature depolarizations earlier at the distal crista catheter, positioned at the RA-SVC junction.
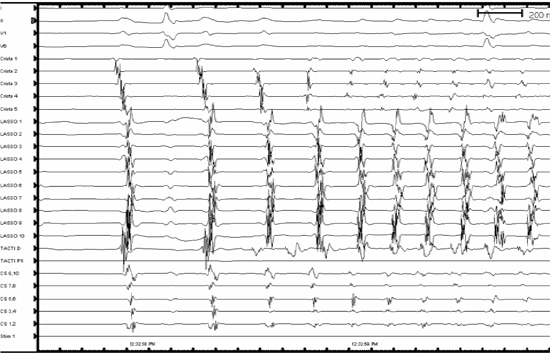
Figure 2. Intracardiac recordings with the Lasso catheter advanced into the SVC, the ablation catheter in the RA and the crista catheter along the RA free wall with the tip in the SVC-RA junction. AF can be observed in the SVC, while both atria are in an organized AT.
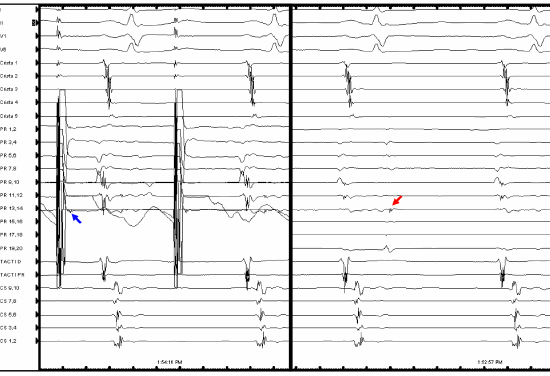
A decision was made to isolate the SVC. High-output pacing to delineate the course of the phrenic nerve revealed significant close proximity to the region of planned ablation. Therefore, using an irrigated ablation catheter with force sensing capabilities (TactiCath, St. Jude Medical, Minneapolis, MN), radiofrequency energy was applied around the SVC ostium distant to the course of the phrenic nerve, starting at the posterolateral region. After only five 20-second contiguous lesions (25 Watts), SVC isolation was achieved, resulting in termination to sinus rhythm, while the SVC remained in AF [Figure 3]. No acute SVC reconnection was demonstrated with Adenosine 12 mg IV or with Isoproterenol infusion up to 12 mcg/min, and no other non-PV triggers were identified. After 7 minutes, AF within the SVC spontaneously terminated. After spontaneous AF termination within the vein, presence of dissociated SVC firing was documented and exit block was further demonstrated by pacing from the Lasso catheter [Figure 4].
Figure 3. ISVC isolation by segmental ablation at the vein ostium. Isolation resulted in immediate AT conversion to sinus rhythm, while the ISVC remained in AF. The red dots represent radiofrequency lesions and the yellow dots represent areas of phrenic nerve capture with high-output pacing.
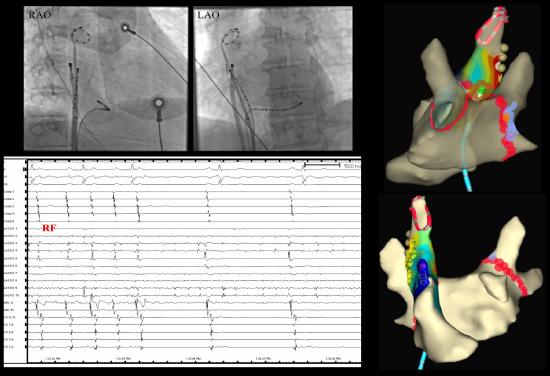
Figure 4. Exit block in the SVC demonstrated by pacing from the Lasso catheter (left panel, sleeve capture marked with blue arrow) and by the presence of spontaneous dissociated potentials in the SVC (right panel, red arrow).
Myocardial sleeves may extend from the RA to the SVC [5] and several studies show that the SVC is an importance source of non-PV triggers in paroxysmal AF [6]-[8]. Myocardial extensions in the SVC harbour ectopic pacing cells that can depolarize by means of abnormal automaticity or afterdepolarization, creating the substrate for atrial arrhythmias, such as AT or AF [9].
This case shows that, in addition of being a source of AF-triggering ectopies, the SVC may contain enough myocardial tissue to sustain AF within the vein. The coexistence of AF within the SVC and organized AT in both atria suggests a discrete breakthrough area between the vein and RA, confirmed in this case by the quick SVC isolation after limited segmental ablation. This resulted in immediate termination of the AT and no reinduction of atrial arrhythmias despite atrial pacing and high-dose isoproterenol.
Electrical disconnection of the SVC can be effectively achieved in most cases by segmental or circumferential ablation [9],[10]. Potential risks of SVC isolation derive from the vicinity of structures such as the sinus node and the phrenic nerve. Before ablation the course of the phrenic nerve should be carefully delineated with high-output pacing and zones with diaphragmatic capture must be avoided to prevent phrenic nerve palsy.






