Reduced P-wave Voltage in Lead I is Associated with Development of Atrial Fibrillation in Patients with Coronary Artery Disease
Bryce Alexander1, Sohaib Haseeb1, Henri van Rooy,3, Gary Tse2, Wilma Hopman1, Manuel Martinez-Selles3, Antoni Bayés de Luna4, Göksel Çinier5, Adrian Baranchuk1
1Division of Cardiology, Queen’s University, Kingston, Ontario, Canada.22Department of Medicine and Therapeutics, Li Ka Shing Institute of Health Sciences, Faculty of Medicine, The Chinese University of Hong Kong, New Territories, Hong Kong.3Servicio de Cardiología, Hospital Universitario Gregorio Marañón, CIBERCV, Universidad Europea, Universidad Complutense, Madrid, Spain.4Institut Català Ciències Cardiovasculars (ICCC). Hospital de la Santa Creu i de Sant Pau. Barcelona. Spain.5Dr. Siyami Ersek Thoracic and Cardiovascular Surgery Center Department of Cardiology, Kadikoy, Istanbul, Turkey..
Reduced P-wave voltage in lead 1 (PVL1) has been associated with atrial fibrillation (AF) recurrence.This study sought to determine the association between reduced PVL1 and AF in the NSTEMI population and the correlation between reduced PVL1 and interatrial block (IAB)/coronary artery disease (CAD).
Data were recorded for clinical, echocardiographic, angiographic, electrocardiographic and outcome variables. Patients were followed for a minimum of one year. Chi-square tests, independent samples t-tests and one-way ANOVA were used for the analysis, which was done using IBM SPSS
A total of 322 consecutive patients were included in the analysis. Patients with new-onset AF had a significantly lower PVL1 (0.085 ± 0.030mV vs. 0.103 ± 0.037mV; p=0.007). There was a significant difference in mean PVL1 between those with no IAB, partial IAB and advanced IAB (p = <0.001). Those with any type of IAB had a significantly lower mean PVL1 than those without (0.094 ± 0.032 mV vs. 0.106 ± 0.038 mV; p=0.005). Patients who developed AF had a significantly longer P-wave duration (126 ± 20ms vs. 119 ± 17ms; p=0.022). Patients with IAB were more likely to develop new-onset AF (15.4% versus 7.5%, p=0.025). There were significant co-linear associations between reduced PVL1 and IAB (p=0.005); reduced PVL1 and diffuse CAD (p=0.031) and IAB and diffuse CAD (p=0.022)
Reduced PVL1 and IAB are associated with new-onset AF in patients with NSTEMI. Reduced PVL1 and IAB are correlated with each other indicating a possible common underlying mechanism. Both parameters are associated with CAD.
Key Words : Interatrial block, atrial fibrillation, P-wave voltage, NSTEMI..
Correspondence to: Adrian Baranchuk, MD FACC FRCPC FCCS
Professor of Medicine
Cardiac Electrophysiology and Pacing
76 Stuart St
Kingston General Hospital K7L 2V7
Queen's University
Reduced P-wave amplitude in lead I (PVL1) has recently been shown to be associated with recurrence of atrial fibrillation (AF) [1]. In this study, conduction was shown to be displaced in the Bachmann region in patients with lower P-wave voltages using left atrial voltage and activation maps. A possible mechanism for the higher rates of AF recurrence in patients with reduced PVL1 was proposed to be abnormal interatrial conduction along the Bachmann region, the same mechanism as believed to underlie interatrial block (IAB).[1] Interatrial block has previously been shown to be associated with atrial fibrillation in multiple cardiac populations. [2-13] The P-wave represents atrial depolarization and as such is an indirect measure of atrial conduction.[14] With normal anatomy, in sinus rhythm, the P-wave initiates at the sino-atrial node and travels inferiorly through the right atrium via the intra-atrial conduction pathways and most commonly crosses the interatrial septum superiorly via the Bachmann region, a broad muscular set of fibers.[15-18] Partial interatrial block (IAB) results from a delay of conduction on this interatrial pathway at the Bachmann region. When this pathway is completely blocked, the right atrium is activated cranio-caudally; however, the left atrium is depolarized from the level of the coronary sinus to the posterior and superior region (retrograde activation) producing the classic biphasic P-wave of advanced IAB.[19] IAB is clinically important due to its correlation with the development or recurrence of AF in various cardiac populations.[2-13] While the exact pathology underlying the conduction abnormalities seen in IAB have not yet fully been determined it has been hypothesized that electrical remodeling and fibrotic atrial remodeling due to reduction of the blood supply to the Bachmann region may play a key role.[20-23] In support of this, IAB has been shown to be associated with diffuse coronary artery disease (CAD).[11] This study sought to determine the association of reduced PVL1 with development of AF in a population of patients with NSTEMI and its correlation with IAB and diffuse CAD.
.
Electronic records of a consecutive cohort of patients at Kingston General Hospital who had presented with a NSTEMI between November 2013 and August 2015 and had an ECG completed in-hospital as part of their work-up were retrospectively reviewed. Exclusion criteria were (i) prior history of AF (ii) lack of at least one significant coronary artery lesion (>70% occlusion) (iii) any STEMI within 90 days prior to the NSTEMI, (iv) significant valvular disease or cardiomyopathy and (v) any device pacing the atrium (vi) active hyperthyroidism.
Electrocardiogram, echocardiogram and angiogram parameters
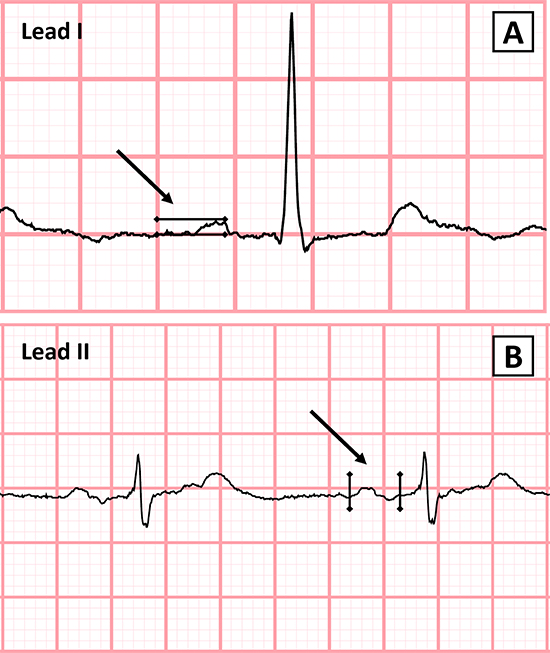
ECGs were scanned at 300 dpi and blindly analyzed using ICONICO semi-automatic calipers. PVL1 was measured from the peak of the P-wave to the isoelectric line of the TP interval (Figure 1a). This method has been previously described and validated with high levels of agreement in both interobserver and intraobserver variability.[1],[24] P-wave onset was defined as the first upward or downward deflection from the isoelectric baseline and the P-wave offset as the return of the waveform to the baseline (Figure 1b). P-wave duration measurement has been previously described and validated.[25] Partial IAB was defined as a P-wave ≥120ms while advanced IAB was defined as a P-wave ≥120ms with biphasic (±) morphology in the inferior leads (II, III and aVF) according to the most recent consensus definition.[19] Reduced PVL1 was defined as a P-wave voltage in lead I less than 0.10 mV. Echocardiographic and angiographic data were taken from clinical reports. Atrial fibrillation was evaluated through review of medical records, EGG’s and holter monitors. AF ≥ 6 minutes’ duration was considered as outcome.[26]
Figure 1a.
Data were collected in Excel and imported into IBM SPSS (version 24.0 for Windows) for statistical analysis. Data were initially described using means and standard deviations for continuous data, and frequencies and percentages for categorical data. This was followed by a univariate analysis to assess the association of the collected data with the
outcome, using one-way ANOVA and independent sample t-tests for the continuous data and chi-square tests (Pearson or Fisher's Exact as appropriate) for the categorical data.
A total of 322 consecutive patients were included in the analysis. The population was 72.3% male, the mean age was 65.4 ± 11.9 years, the mean ejection fraction was 55.2 ± 12.7% and the mean left atrial diameter was 38.7 ± 6.0mm. Population characteristics are presented in [Table 1]. The prevalence of PVL1 less than 0.10 mV (reduced PVL1) was 50.3%, PVL1 between 0.10 and 0.20 mV was 48.8% and PVL1 > 0.20 mV was 0.9%. The prevalence of partial IAB was 31.7% and the prevalence of advanced IAB was 6.5%. The incidence of new onset AF within one year was 10.6%. The population was normally distributed in terms of P-wave voltage and duration
Table 1. Population characteristics
| Clinical Variable |
Value (n = 322) |
| Age (years) ± SD |
65.4 ± 11.9 |
| Male sex |
233 (72.3%) |
| BMI (kg/m2) |
29.8 ± 6.6 |
| Partial interatrial block |
102 (31.9%) |
| Advanced interatrial block |
21 (6.5%) |
| Prior smoker |
204 (63.4%) |
| Hypertension |
232 (72.0%) |
| Prior smoker |
204 (63.4%) |
| Dyslipidemia |
182 (56.5%) |
| Diabetes |
104 (32.3%) |
| Prior transient ischemia attack or stroke |
35 (10.9%) |
| Obstructive sleep apnea |
37 (11.4%) |
| Pulmonary disease |
49 (15.2%) |
| Prior known coronary artery disease |
118 (36.6%) |
| Congestive heart failure |
15 (4.7%) |
| Previous cardiac surgery |
43 (13.4%) |
| Prior atrial flutter |
3 (1.0%) |
| Left ventricular ejection fraction (%) |
55.2 ± 12.7 |
| Body surface area (m2) |
1.97 ± 0.22 |
| Left atrial diameter (mm) |
38.7 ± 6.0 |
| Right atrial volume indexed to BSA (ml/m2) |
22.6 ± 15.6 |
Associations with Atrial Fibrillation
Participants who developed new-onset AF within one year had a significantly lower PVL1 (0.085 ± 0.030mV vs. 0.103 ± 0.037mV; p=0.007) and significantly longer P-wave duration (126 ± 20ms vs. 119 ± 17ms, p=0.022) than those who did not develop AF ([Table 2]). Multivariate logistic regression analysis was not completed due to substantial co-linearity between the three variables in the model (IAB, reduced PVL1 and diffuse CAD defined as the presence of two or more significant coronary artery lesions in the same patient). There were significant co-linear associations between reduced PVL1 and IAB (p=0.005); reduced PVL1 and diffuse CAD (p=0.031) and IAB and diffuse CAD (p=0.022).
Table 2. Difference in IAB Categories between P-Wave Voltage Categories
|
Any IAB ( |
either partial or advanced) |
|
|
Absent (n = 199) |
Present (n = 123) |
P-Value |
| P-Wave Voltage (mV) |
0.106 ± 0.038 |
0.094 ± 0.032 |
0.005 |
|
Advanced |
IAB |
|
|
Absent (n =301) |
Present (n = 21) |
|
| P-Wave Voltage (mV) |
0.103 ± 0.362 |
0.074 ± 0.029 |
<0.001 |
|
New Onset Atrial |
Fibrillation |
|
|
Absent (n =288) |
Present (n = 34) |
|
| Mean P-Wave Voltage (mV) |
0.103 ± 0.037 |
0.085 ± 0.030 |
0.007 |
| Mean P-Wave duration (ms) |
119 ± 17 |
126 ± 20 |
0.022 |
Correlation of P-Wave Voltage with P-Wave Duration
There was a significant difference of mean P-wave duration between PVL1 categories (<0.10mV, 0.10-0.20mV and >0.20mV) (p = 0.009) ([Table 3]). This difference favored increased P-wave duration with decreased PVL1 category. There was also a significant difference in the presence of advanced IAB between the PVL1 categories (p = 0.014) and in the prevalence of any IAB (p = 0.035) ([Table 4]).
Table 3. Difference in P-Wave Voltage and Duration by IAB and Voltages Categories
| Inter Atrial Block Category |
Mean P-wave Voltage (mV) |
P-Value |
| No interatrial block |
0.106 ± 0.038 |
|
| Partial interatrial block |
0.098 ± 0.031 |
<0.001 |
| Advanced interatrial block |
0.074 ± 0.029 |
|
| Voltage Category |
Mean P-wave Duration (ms) |
P-Value |
| <0.10 mV |
122.1 ± 18.1 |
|
| 0.10 - 0.20 mk |
117.0 ± 16.0 |
0.009 |
| >0.20 mV |
105.0 ± 2.6 |
|
Table 4. Method for the Measurement of P-Wave Duration and Amplitude
|
Any IAB ( |
either partial or dvanced) |
|
| P-Wave Voltage |
Absent (n = 199) |
Present (n = 123) |
P-Value |
| <0.10 mV |
90 (45.2%) |
72 (58.5%) |
|
| 0.10 - 0.20 mV |
106 (53.3%) |
51 (41.5%) |
0.035 |
| >0.20 mV |
3 (1.5%) |
0 (0.0%) |
|
|
Advanced IAB |
IAB |
|
|
Absent (n = 301) |
Present (n = 21) |
|
| <0.10 mV |
145 (48.2%) |
17 (81.0%) |
|
| 0.10 - 0.20 mV |
153 (50.8%) |
4 (19.0%) |
0.014 |
| >0.20 mV |
3 (1.0%) |
0 (0.0%) |
|
Correlation of IAB Category with P-Wave Voltage
There was a significant difference of mean PVL1 between those with no IAB, partial IAB and advanced IAB (p = <0.001) ([Table 3]). This difference favored decreased PVL1 with increased severity of IAB category. Patients who had advanced IAB had a significantly lower mean PVL1 than those without advanced IAB (0.074 ± 0.029 mV vs. 0.103 ± 0.362 mV; p=<0.001). Patients who had any type of IAB had a significantly lower mean PVL1 than those without IAB (0.094 ± 0.032 mV vs. 0.106 ± 0.038 mV; p=0.005) ([Table 2])
Reduced PVL1 was found to be significantly associated with the development of new-onset AF in this population. In addition, reduced PVL1and IAB were found to be significantly correlated with each other. It is plausible that reduced PVL1 and IAB may be associated with the same pathological process leading to increased P-wave duration and reduced voltage, namely atrial fibrosis. Park et al. have recently demonstrated a significant correlation between reduced PVL1 and displaced conduction in the Bachmann region using left atrial voltage and activation maps.[1] Atrial fibrosis delays cardiac electrical conduction and reduces voltage, phenomena which have been well described previously.[27-31] Since the P-wave voltage depends on the direction of electrical propagation relative to the axis of the lead being measured and the myocardial mass and intervening substrates; it has been proposed that reduced P-wave voltage may be a result of an altered atrial conduction pattern and decreased myocardial mass due to atrial fibrotic scarring and increased degree of electro-anatomical remodeling.[1] It has recently been shown that diffuse CAD is associated with IAB and development of AF in the NSTEMI population.[11] In this current study, both reduced PVL1 and IAB are also significantly correlated with diffuse CAD. Therefore it is possible that the mechanism underlying both decreased PVL1 and IAB is fibrosis of the atria, particularly in the Bachmann region.[32],[33]
This study was retrospective in nature and as such may present inherent bias. AF was determined by clinical examination, ECG and Holter monitor reports; thus silent AF episodes may not have been recorded.
Reduced PVL1 is associated with new-onset AF in the NSTEMI population. In addition, PVL1 and IAB are significantly correlated with each other and with diffuse CAD. While the exact mechanism responsible for each have yet to be worked out, it is possible that the underlying cause could stem from fibrosis of the atria






