Leaks after left atrial appendage ligation with Lariat device: Incidence, pathophysiology, clinical implications and methods of closure- A case based discussion
Bharath Yarlagadda, Valay Parikh, Tawseef Dar, Dhanunjaya Lakkireddy
Division of Cardiovascular Diseases, Cardiovascular Research Institute, University of Kansas Hospital & Medical Center, Kansas City, KS.
Catheter based left atrial appendage (LAA) closure techniques are emerging as a promising alternative for stroke prevention in patients who cannot tolerate oral anticoagulation. Lariat procedure involves percutaneous catheter based epicardial ligation of the LAA with a suture via an endo-epicardial hybrid approach. It offers the advantage of not leaving behind a focus for thrombus formation or embolization. Similar to surgical ligation of the left atrial appendage, Lariat ligation is limited by leaks in a small percentage of patients. The incidence of leaks is variable and can be seen in the immediate post procedure period or during follow up. The electrical and mechanical implications of leaks are still under debate. In this review, we discuss the incidence, pathophysiology, clinical implications and methods of closure of leaks after Lariat. In the end, we present a case of a Lariat leak closed with an Amplatzer septal occluder.
Key Words : Atrial fibrillation (AF), Left atrial appendage (LAA), Left atrial appendage closure (LAAC), LAA ligation, Lariat, Leaks after Lariat procedure.
Correspondence to: Dhanunjaya Lakkireddy, MD, FHRS
Professor of Medicine,
Mid America Cardiology,
University of Kansas Hospital,
Kansas City, KS 66160.
Tel: 913-588-9406
Fax: 913-588-9770
Email: dlakkireddy@kumc.edu
Atrial fibrillation (AF) remains the most common sustained arrhythmia in the United States affecting more than 6.1 million adults [1]. It is associated with significant morbidity and mortality as it is an independent risk factor for stroke[2]. Thrombus in the left atrial appendage (LAA) contributes to 90% of AF related strokes[3]. Oral anticoagulation(OAC) can reduce the risk of stroke by up to 64%[4]. However, their use is contra-indicated in some patients because of significant risk of bleeding[5]. Procedural exclusion of the LAA is an alternative in patients with high risk of bleeding. Recent studies also suggest LAA as a non-pulmonary vein focus of origin of AF [6]. Epicardial based exclusion procedures can electrically isolate the LAA and there might be a benefit of reducing AF burden in addition to stroke prevention. Surgical separation of the LAA during coronary artery bypass grafting or valve replacements has been around for a long time [3]. Minimally invasive surgical techniques like AtriClip (AtriCure Inc. Cincinnati, Ohio) are also available [7], [8]. Historically, surgical techniques including off pump suturing, endocardial suturing and stapling have been associated with significant incomplete closure, stumps and increased risk of systemic thromboembolism [9].
Several nonsurgical percutaneous LAAC techniques were developed recently. The Watchman device (Boston Scientific Corp, Minneapolis, MN) which is deployed after trans-septal puncture via percutaneous catheter-based delivery system is one of them. The PROTECT-AF trial showed non inferiority of the Watchman device in preventing strokes when compared to warfarin in AF patients who cannot tolerate anticoagulation[10]. Lariat suture ligation (SentreHEART Inc, Redwood, CA) is another LAAC technique. It allows for percutaneous catheter based epicardial ligation of the LAA with a suture via an endo-epicardial hybrid approach[11].
Similar to surgical closure techniques (between 10 and 80%)[12], percutaneous LAAC techniques are limited by leaks in a small percentage of patients. Leaks can develop at the time of implant due to incomplete closure or de-Novo during follow up due to tissue remodeling. Their clinical implications are still under debate. With some reports suggesting an association of leaks with thromboembolism, it’s an area of growing interest. In this manuscript we describe the incidence, pathophysiology, clinical implications and methods of closure for post Lariat leaks.
Incidence and types of leaks
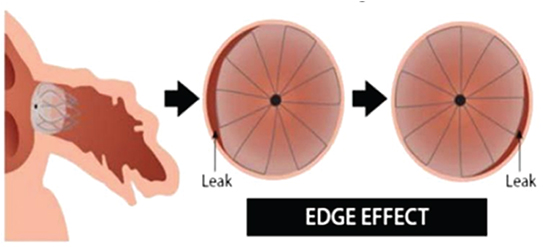
Several studies have shown that leaks are a complication of percutaneous LAAC devices [10], [13], [14]. The incidence and characteristics of leaks vary based on the procedure. With endocardial plug type devices a circular devices attempts to occlude a non-circular orifice with variable dimensions thereby producing the “Edge effect” [13][Figure 2].Depending on the compliance and remodeling capability of the LAA whether the tissue around the device remains snug fit or not is variable. In the case of epicardial systems there are two types of issues – 1. Central leaks due to suture not ligating the entire neck of the LAA and 2. Stump – long piece of the LAA neck or base left behind. We have previously described the leaks after Lariat procedure as concentric and central owing to the “Gunny sack effect” caused by suture ligation around the LAA [13][Figure 1].
Figure 1. Shows the “Gunny sack effect” describing a concentric leak after Lariat procedure. Image adapted from the study by Pillarisetti et al
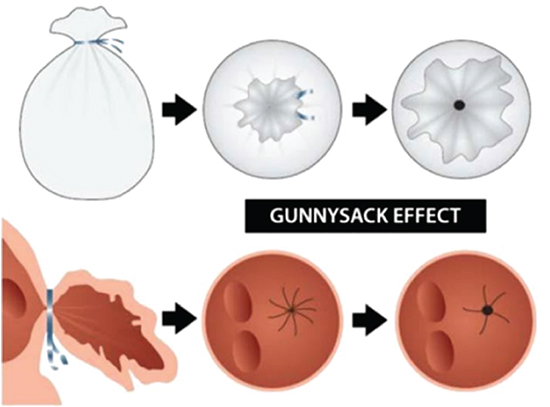
Figure 2. Shows the “Edge effect” describing a peri-device leak after Watchman device. Image adapted from the study by Pillarisetti et al
The incidence of leaks after Lariat procedure range from 0% to 24% [13], [15]-[19][Table 1]. The large variation in the incidence rates are likely due to an evolving technique, site of suture application and lack of standardized imaging for identifying leaks. The leak size is determined by the final diameter of the suture loop used and whether repeated tensuring was done after the initial suture deployment or not. If the suture is deployed too close to the atrium, it can result in a larger suture loop with a significant amount of bunched up tissue that may subsequently unfurl opening up the central portion of the suture loop. In a recent study, one of the factors which led to higher reporting of leaks was the use of 3D TEE[14]. In this study 3 additional patients were found to have leaks which were missed on traditional 2D TEE.
Table 1. Incidence rates of leaks after Lariat suture ligation of the LAA.
| Author (year)[reference #] |
N |
Acute |
Early(<6m) |
Late(6-12m) |
| Bartus et al (2013)[15] |
85, 81, 65 |
3(4%) |
4(5%) |
1(2%) |
| Massumi et al (2013)[16] |
20, 17, 17 |
0(0%) |
1(6%) |
1(6%) |
| Miller et al (2013)[18] |
41, 41 |
3(7%) |
10(24%) |
- |
| Price et al (2013)[19] |
145, 63 |
5(8%) |
13(20%) |
- |
| Pillarisetti et al (2015)[13]
|
259, 259, 259 |
5(2%) |
33(13%) |
33(13%) |
| Gianni et al (2016)[14] |
98, 96, 96 |
5(5%) |
14(15%) |
19(20%) |
| Lakkireddy et al(2016) |
682, 480, 480 |
13(1.8%) |
31(6.5%) |
31(6.5%) |
*N=Number of patients in each study at the time of procedure, 6months and 12months.
Leaks were reported as major (≥5mm) or minor (≤5mm) based on the size for the endocardial closure devices. Majority of leaks after the Lariat procedure were ≤2mm and rarely >5mm [13]. The definition of an acceptable versus unacceptable leak is still up for debate. Leaks can occur in the immediate post procedure period or can be observed during follow up. [Figure 3] and [Figure 4] show acute and long term closure rates in various studies. In a prospective study by Pillarisetti at al which included 259 patients, 5 patients (2%) had small leaks at the time of implantation, 33 patients (13%) had leaks at 1-3 months and 9 months follow ups. In a retrospective study by Gianni et al, 98 patients underwent Lariat suture ligation and followed with 3D TEE immediately post procedure, at 6 months and at 12 months. Acute leaks (at the time of the procedure) were seen in 5 patients (5%). Of these 5 patients, only 2 persisted at 6 months follow up. Among patients with no acute leaks, early leaks (evident at or before 6 months follow up) were identified in 12(13%) patients and late leaks (diagnosed after the 6 months follow up) were identified in 2 patients (5%). In this study, a total of 14(15%) and 19(20%) patients had leaks at 6 months and 12 months follow up respectively [14]. In a recent large multicenter evaluation of 682 patients reported by our group, acute leaks less than 2mm were seen in 13 patients (1.8%). Follow up TEE was available in 480 patients, which showed leaks between 2-5mm in 31 patients (6.5%)[20]. Acute leaks are likely because of suboptimal tightening of the suture. They might spontaneously close due to endothelialization or fibrosis, especially if size is <3mm. Early or late leaks maybe due to knot loosening due to tissue unfurling or tissue necrosis at the site of suture as observed with surgical ligation [21]. They are less likely to close spontaneously in our experience.
Figure 3. Shows the acute closure rates with Lariat device in various reported studies
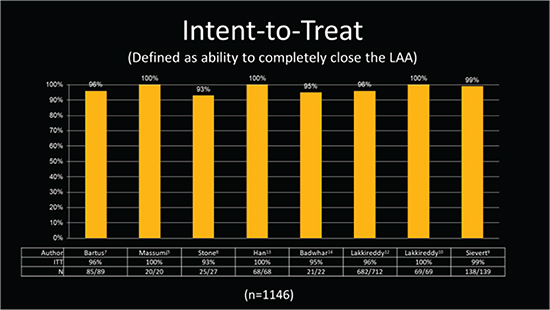
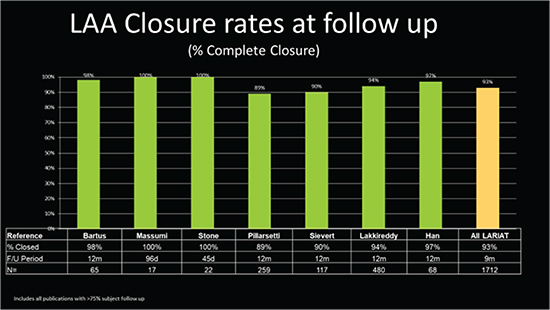
Figure 4. Shows the longterm closure rates during follow up. > 75% of patients had follow up TEEs in these studies
Pathophysiology of leaks in Lariat system
The following factors play a very important role in the presence or absence of leaks.
. Size of the LAA at the site of closure – large necks often result in incomplete closure as there is too much tissue to approximate
. Proximity to the atrial wall - The closer one gets to the atrial wall at the base more tissue gets bunched up into the suture and often prevents it from tensuring right. Over a period of time the tissue inside the loop remodels and unfurls to open a communication proximal and distal to the ligature.
. Appropriate deployment and tensuring of the suture - If the device is not lined up properly and the tissue is not tensured the chances of leaks is high.
. False closure due to the pressure from the device - Occasionally, the magnets might not align and are attached outside the LAA. If the operator doesn’t realize the issue and moves the delivery device forwards deploying the suture and falsely compressing the LAA resulting in pseudo closure. An atrial angiogram should always be performed once the nitinol loop comes off of the LAA prior to withdrawing the sheath to the right side.
. Incomplete closure due to basal lobes - In a small percentage of patients the proximal portion of the LAA may have separate lobes and the suture may simply ligate one of the lobes leaving behind the others untreated.
Why does a Lariat close the LAA better than a surgical hand knot?
In vast majority of hand knots that were done during open heart procedures, the heart was on a heart-lung pump with LAA being flaccid. It is very hard to tie a suture around flaccid piece of tissue. The analogy one can try here is that of a deflated vs inflated balloon and applying a knot around it. It’s a lot easier to tie a self-retaining knot around the neck of an inflated balloon and subsequent tensuring will result in making it tighter. The Lariat suture delivery follows this very principle and has shown that the closure rates are dramatically higher than what has been described in surgical literature [Figure 5]. Once the self-retaining suture is deployed, subsequent tensuring of the suture helps to tighten the suture around the tissue, desiccating it further and allowing for the lowest possible suture diameter to close off the neck. So in larger necks it may be necessary to tensure the suture more than once. And confirming closure after the Lariat loop comes off of the LAA is critical to ensure acute closure.
Figure 5. Shows the difference in suture deployment when the target is inflated vs deflated

Clinical Implications of leaks
Successful LAAC with Lariat suture ligation system results in electrical and mechanical isolation of the LAA reducing the risk of stroke and recurrence of AF. There is limited data on the electrical and mechanical implications in patients with leaks following Lariat procedure. This was studied in a recent prospective multicenter study by our group. A total of 91 patients with AF who underwent Lariat suture ligation followed by catheter ablation were studied. Of these, 7 patients had leaks ranging from 1-3mm and 4 patients had leaks between 4-5mm. Morphological characteristics of the LAA remnant (LAAR) were assessed with CT scans obtained pre procedure and at 1 month. Electrical activity of the LAAR was assessed during CA performed within a month from the Lariat procedure. We reported significant reduction in the LAA volumes (66%) and size (67%) however larger leaks had slightly larger LAAR. Of the 4 patients with leaks between 4-5mm, 3 demonstrated electrical activity during CA and were successfully isolated. There was lack of statistically significant correlation between leaks and recurrence of AF at 1 year follow up.
Leaks following surgical exclusion of the LAA have been reported to be associated with thromboembolism. Continued anti-coagulation is recommended in these patients because of this risk. This association with thromboembolism is poorly understood with leaks following percutaneous LAAC techniques. Theoretically, in patients with Watchman device the implant can act as a nidus for thrombus formation and stroke in the absence of anti-coagulation or antiplatelet therapy. In PROTECT-AF study, albeit leaks with associated thrombi, there was no association between stroke and the presence or size of the leaks[10]. Similar findings were observed in the subgroup of patients with Watchman device in the study by Pillarisetti et al [13]
There is no randomized controlled data for Lariat looking at the impact of leak on the overall risk of stroke. It is clear while the presence of a leak may not increase the stroke risk but complete closure doesn’t assure the elimination of stroke risk. Even though epicardial exclusion of the LAA with Lariat suture does not leave a nidus for thrombus formation there still is a risk in the immediate post procedural period. Thrombus at the closure site has been reported in 2.5% Lariat cases irrespective of the closure. This is thought to be secondary to local inflammatory changes caused by tissue infarction due to application of the suture [13]. In a recent retrospective study with 98 patients, 5 developed thromboembolisms. Three of the 5 were found to have leaks on 3D TEE, 2 patients in which the TEE was not available presented with thromboembolic events. None of the patients without leaks developed thromboembolic events [14]. In 2 of 3 patients with leaks on 3D TEE they were not detected on 2D TEE. This observation questions the role of various imaging modalities in identifying leaks. This association with thromboembolism was not reproducible in a recent multicenter prospective study which followed 259 consecutive patients with 2D TEE who underwent LAAC with Lariat suture [13]. There is a significant uncertainty regarding the association between leaks and thromboembolism.
Most operators choose to resume anticoagulation/antiplatelet agents in patients with leaks after percutaneous LAAC in the absence of contraindications. This might not be the case for most patients who undergo Lariat procedure because of their high bleeding risk. The other alternative is to pursue repeat exclusion of the LAA. Before consideration for exclusion procedures it’s important to keep in mind that leaks ≤2 mm might spontaneously close [15], [20] and can be observed, while leaks ≥3mm are less likely to close.
Several endocardial occlusion devices are being used for closure of leaks after surgical or non-surgical LAA exclusion [21]-[23]. The concentric and central location of leaks seen after Lariat suture ligation makes it feasible for septal closure devices. Because of the narrow neck of the LAA conventional closure devices like Watchmen device cannot be used [21]. Amplatzer septal occluder (ASO), originally designed for the closure of atrial septal defects, is now being used off label for closing LAA leaks. In a recent case series, we reported 5 patients with leaks ranging from 3.5 mm - 5 mm after Lariat procedure successfully closed with ASO device [21]. All patients were on anti-platelet agents (clopidogrel 75mg qday) for 6 weeks until endothelialization of the device as per standard practice. There was no residual leak noted at 3 months follow up. ASO is a self-expandable device made of nitinol mesh and fabric patches delivered through a transseptal sheath positioned in the LAA. Mosley et al reported successful closure of 3 late Lariat leaks using Amplatzer vascular plug 4(AVP-4). AVP-4, approved to close AV fistulas, is a double lobed retractable nitinol based device which is deployed through a 4-5 French diagnostic catheter [22]. There was another case of incomplete LAA closure that was closed with an Atriclip using a minimally invasive technique. In this case, only the distal lobe of the bilobed LAA was closed with the Lariat leaving behind a large proximal lobe [24]. Alternative approaches like coils or other septal occluders (e.g., GORE Helex septal occluder[GORE medical, Flagstaff, AZ]) can also be used[25]. Several exclusion techniques were described anecdotally. A repeat Lariat suture was used to close a leak in one recent case report [21]. This can be difficult because of potential adhesions from pericardial inflammation caused by the initial pericardial access and suture.
How to close a leak using ASO: A stepwise descriptive
A 75 year old female patient with permanent AF status post multiple left antral ablations who suffered an embolic CVA (CHADSVASC of 5) while on Coumadin underwent Lariat suture ligation. She had a large LAA with a neck diameter of 4cm. There was significant difficulty encircling the whole appendage and required multiple attempts during the procedure. She had a 1mm residual leak at the end of the procedure on TEE. She was subsequently found to have a 4 mm leak at her 3 month follow up. Because of her high stroke risk it was decided to pursue closure of the leak with ASO. After correct patient identification, an informed consent was obtained after discussing the risks and benefits of the procedure. The procedure was performed in a hybrid catheterization lab under general anesthesia. A TEE was performed prior to gaining access to exclude LAA thrombus and to assess the dimension of the neck of the leak between the LAA and the LA. After obtaining femoral vein access, transseptal access was obtained by using a Brockenbrough needle and an 8.5Fr SL1 sheath (St.Jude Medical, St Paul, MN) under TEE and fluoroscopic guidance. A left atrial appendogram was obtained in the right anterior oblique and left anterior oblique views to assess the dimensions and characteristic of the leak between the LAA and LA.
Complete opacification of the LAA was obtained with the appendogram with neck diameter measuring 4 mm. The SL1 sheath was exchanged for an 8.5 Fr Mullins sheath. A soft-tipped 0.035-inch wire was passed across the neck into the LAA under fluoroscopic and TEE guidance. The distal tip of the Mullins sheath was positioned just beyond the neck.
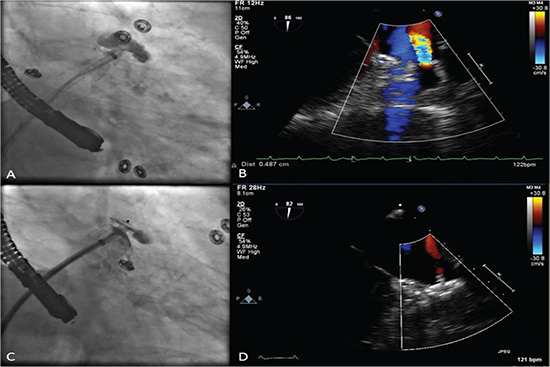
A 5 mm ASO was chosen based on the patients LAA leak. The ASO device was advanced through the sheath beyond the neck. It was unsheathed such that the outer disk was deployed inside the LAA and the inner disk on the LA aspect of the neck with the waist of the device exactly aligned with the neck. A “tug test” was performed to ensure the stability of the device. Angiography and TEE were used to confirm the absence of any residual leak across the device [Figure 6]. The patient was started on clopidogrel 75mg qday for 6 weeks until endothelialization of the device as per standard practice. There was no residual leak noted at 3 months follow up on TEE.
Figure 6. Panel A shows remnant connection between left atrium and LAA after contrast injection. Panel B shows the same leak on TEE. Panel C shows ASO device obliterating the remnant connection between the LA and the appendage after contrast. Panel D shows TEE images of the ASO device in situ. LAA= Left atrial appendage, ASO = Amplatzer septal occluder, TEE = Transesophageal echocardiogram
Post procedural anticoagulant or antiplatelet regimen after device closure of a leak
If the patient is able to take oral anticoagulation at least in the short term, should be treated with one for at least 6 weeks to allow for endothelialization followed by dual antiplatet therapy (DAPT). If OAC is not an option DAPT for at least 6 months is important. After 6 months ASA 81 mg may suffice. Periodic TEE monitoring may be important to understand the long term implications of device related thrombus in these cases is still not well understood.
Leaks are a known complication after Lariat suture ligation. They can be detected at the time of procedure or during follow up. There is no correlation between leaks and recurrence of AF. There is limited data on the relationship between leaks and thromboembolism. Because of the possible association with thromboembolism patients should be followed up long term with serial TEE imaging. Anticoagulation should be resumed if feasible or repeat percutaneous closure with endovascular or epicardial techniques should be pursued if there is a high risk of stroke. The concentric and central nature of the leak after Lariat makes it feasible to use septal closure devices to close a leak.






