New-onset Heart Failure With Atrial Fibrillation: A Distinct Type of Cardiomyopathy?
Vinay Mehta1*, Alexander Albers2,3, Maharaj Singh3,t, Ana Cristina Perez Moreno3, Timothy E. Paterick4
1Department of Electrophysiology, Aurora BayCare Medical Center, 2845 Greenbrier Road, Ste. 330, Green Bay, WI 54311 USA.2Department of Clinical Research, Aurora BayCare Medical Center, 2845 Greenbrier Road, Room 519, Green Bay, WI 54311 USA.3Aurora Research Institute, Aurora Health Care, 945 N. 12th St., Milwaukee, WI 53233 USA.4Department of Cardiovascular Disease, Aurora BayCare Medical Center, 2845 Greenbrier Road, Ste. 330, Green Bay, WI 54311 USA.*Dr. Mehta’s current affiliation is Nuvance Health, Danbury, Connecticut.tDr. Singh’s current affiliation is School of Dentistry, Marquette University, Milwaukee, Wisconsin.
There is limited research comparing demographic and clinical characteristics between patients who present with atrial fibrillation (AF) and new-onset cardiomyopathy (CM) to patients with new-onset CM without dysrhythmia. We aimed to evaluate clinical characteristics and outcomes in patients with new-onset CM with and without AF and to report their real-world treatment.
The study population was identified using patient records from our healthcare system from January 1, 2012 to September 30, 2016. Patients with a left ventricular ejection fraction ≤40% without a prior history of CM were divided into two groups; those with an antecedent or concomitant diagnosis of AF (AF-CM group) and those with no history of dysrhythmia (CM group). Patients in the AF-CM group (n=196) were older, more likely to be male, had a higher burden of comorbidities but lower levels of cardiac biomarkers, and had lower voltage on surface electrocardiogram than the CM group (n=197). In AF-CM, symptom onset was insidious, leading to a higher likelihood of outpatient diagnosis; 88.3% of AF-CM patients presented with atypical symptoms of AF. The AF-CM group had higher mortality on follow-up. Only 8.7% of patients in this group underwent an ablation procedure. Women, those with a history of coronary artery disease, and older patients were less likely to receive a cardioversion or ablation procedure.
Patients presenting with new-onset CM associated with AF have a markedly different risk factor and demographic profile, clinical presentation, and outcomes. In real-world practice, a minority of patients undergo a rhythm control strategy.
Key Words : Atrial fibrillation, Heart failure, New-onset cardiomyopathy, Ablation.
Vinay Mehta, MD
111 Osborne Street, 3rd Floor
Danbury, CT 06810
This study evaluates differences between new-onset cardiomyopathy (CM) with and without atrial fibrillation (AF). New-onset CM is defined as a left ventricular ejection fraction (EF) ≤40% with no prior history of CM. The distinction between the two CM groups is whether there is a concomitant or preceding history of AF (AF-CM group) or there is no history of concomitant or antecedent AF (CM group). There has been increasing recognition that AF may present with typical or atypical symptoms and often can be classified as asymptomatic 1-4. The prevalence of AF with typical or atypical symptoms in this patient population is not known, and we attempt to answer that question. We also report the real-world treatment pattern for these patients in a large healthcare system.
The local institutional review board approved this study, which was conducted in accordance with the Declaration of Helsinki. Informed consent requirement was waived.
Study Population and Data Collection
Through retrospective review of echocardiographic data in patient charts in Aurora Health Care system’s electronic medical records (EPIC, Verona, WI) from January 1, 2012 to September 30, 2016, we identified patients with new-onset CM with a left ventricular EF ≤40% and no prior history of low EF. Initial data were abstracted by Aurora Research Institute’s EPIC data retrieval team electronically. Both inpatients and outpatients were included in the study. Each patient was manually assessed for inclusion and exclusion criteria by the research coordinators under the supervision of the principal investigator. Patients with any pre-existing evidence of CM based on office notes and/or cardiac imaging were excluded. Patient demographic data, medical comorbidities, admission diagnosis, admission laboratory values, peak troponin values, and voltage based on EKG were collected. EKG voltage was measured utilizing the Sokolow criteria 5, measuring the S wave in V1 plus the R wave in V5 or V6 (whichever was largest). Information about the treatment these patients received both as an inpatient and outpatient was collected. Readmission and mortality data were obtained. An almost equal number of patients were included for each 5% difference in left ventricular EF. An equal number of patients were collected for EF <20%.
Patients with a pre-existing cardiovascular implantable electronic device were excluded, as were patients with a history of any other dysrhythmia, including frequent premature ventricular contractions (PVCs; >2 PVCs on surface EKG, ventricular trigeminy, or more on telemetry). Additional exclusion criteria were unreadable or poor-quality echocardiogram, mortality during inpatient admission, and presence of congenital heart disease.
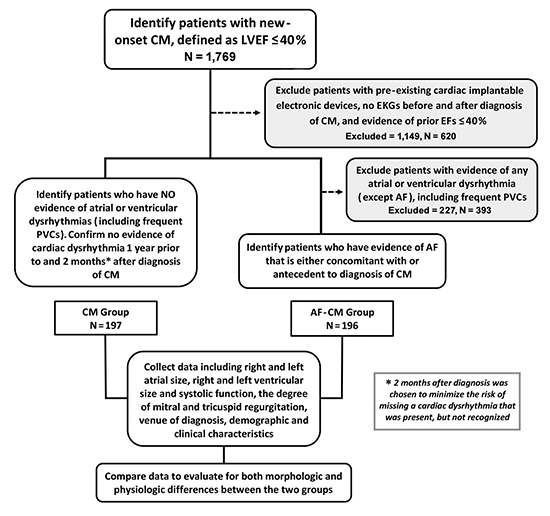
Then, patients were divided into two categories: those with an antecedent or concomitant diagnosis of AF (AF-CM group) and those without a history of any preceding dysrhythmias (CM group). Patients included in the isolated CM group were required to not have had any atrial or ventricular dysrhythmia in the preceding 1 year or the consecutive 2 months after the diagnosis of CM. The consecutive 2 months after the diagnosis of CM was selected as part of this criterion to minimize the likelihood of missing cryptogenic AF or other dysrhythmias in this population. Patients were matched according to left ventricular EF [Figure 1]. All data were stored electronically in a secure and de-identified manner on official Aurora Health Care computer systems.
Figure 1. Study design. AF, atrial fibrillation; CM, cardiomyopathy; EF, ejection fraction; EKG, electrocardiogram; PVC, premature ventricular contraction.
Study subjects were matched for left ventricular EF. Descriptive data are presented in tables as frequencies and percentages and means ± standard deviations. Baseline characteristics were compared among intervention groups by chi-square or Fisher’s exact tests and one-way analysis of variance or Kruskal-Wallis test, accordingly. The association between AF-CM or CM alone with the composite outcome of hospital readmission or death was examined using Kaplan-Meier analysis. Linearity and proportional hazards assumptions were assessed and fulfilled. All P values are reported as 2-tailed, with <0.05 considered to be statistically significant. All statistical analysis was performed using SAS 9.4 (SAS Institute, Cary, NC) or Stata version 15 (StataCorp, College Station, TX).
[Figure 2]
Differences in Demographic Characteristics and Comorbidities
Over a 4-year period, 393 patients with new-onset CM were identified: 196 patients were identified in the AF-CM group, and 197 patients in the CM group.
Figure 2. Prototypical patients. The prototypical patients with new-onset heart failure with (AF-CM Phenotype) and without atrial fibrillation (CM Group) are depicted. AF, atrial fibrillation; BNP, brain natriuretic peptide; CAD, coronary artery disease; CM, cardiomyopathy; HTN, hypertension.
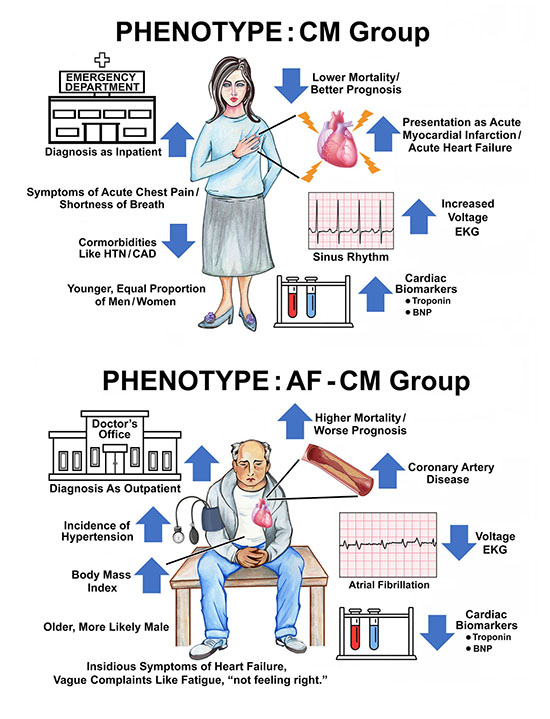
Patients in the AF-CM group, in comparison to the CM group, were older (73.51 years vs. 64.18 years, respectively; P < 0.001), more likely to be male (63.3% vs. 49.2%, respectively; P=0.005), more likely to have a history of hypertension (70.4% vs 53.3%, respectively; P=0.0005), and more likely to have a history of coronary artery disease (33.7% vs 20.8%, respectively; P=0.0042). They were also likely to have a slightly higher body mass index (31.5 vs. 29.8, respectively; P=0.04) [Table 1].
Table 1. Demographic and clinical characteristics.
| Characteristic |
AF-CM group (n=196) |
CM group (n=197) |
P value |
| Age, years |
73.51±12.14 |
64.18±15.98 |
<0.001 |
| Body mass index |
31.5±8.2 |
29.8±7.7 |
0.04 |
| Sex, male |
124 (63.3) |
97 (49.2) |
0.01 |
| Race |
|
|
<0.001 |
| White |
190 (96.9) |
151 (76.7) |
|
| Black/African American |
4 (2.0) |
39 (19.8) |
|
| Others |
2 (1.0) |
7 (3.5) |
|
| Tobacco use |
119 (60.7) |
132 (67.0) |
0.19 |
| Alcohol use |
24 (12.2) |
71 (36.0) |
<0.001 |
| Hypertension |
138 (70.4) |
105 (53.3) |
<0.001 |
| History of PCI |
36 (18.4) |
38 (19.3) |
0.82 |
| Hyperlipidemia |
115 (58.7) |
81 (41.1) |
<0.001 |
| Coronary artery disease |
66 (33.7) |
41 (20.8) |
<0.01 |
| Diabetes mellitus |
59 (30.1) |
57 (28.9) |
0.80 |
| History of drug abuse |
4 (2.1) |
15 (7.6) |
0.01 |
| Outpatient diagnosis |
70 (35.7) |
20 (10.2) |
<0.001 |
| Presenting symptoms |
|
|
<0.001 |
| Congestive heart failure |
128 (65.3) |
82 (41.6) |
|
| Myocardial infarction |
0 (0.0) |
46 (23.3) |
|
| Others/unknown |
68 (34.7) |
69 (35.0) |
|
| Deceased |
62 (31.6) |
44 (22.3) |
0.04 |
| Palpitations on presentation |
23 (11.7) |
3 (1.5) |
<.0.001 |
| LVEF on diagnosis |
|
|
0.99 |
| 36-40% |
43 (21.9) |
42 (21.3) |
|
| 31-35% |
40 (20.4) |
43 (21.8) |
|
| 26-30% |
45 (23.0) |
43 (21.8) |
|
| 21-25% |
33 (16.8) |
33 (16.8) |
|
| ≤20% |
35 (17.9) |
36 (18.3) |
|
Data presented as n (%) or mean±standard deviation.
Differences in Clinical Presentation, Diagnosis Setting, and Myocardial Infarction
A majority of patients in the AF-CM group had an atypical clinical presentation of AF. Only 23 patients (11.7%) had palpitations listed as one of their presenting complaints. A majority (65.3%) of AF-CM patients presented with insidious onset of congestive heart failure (CHF) symptoms. There were no patients in this group who presented with an acute myocardial infarction [Figure 3].
Figure 3. Presenting symptoms. Patient-reported symptoms at the time of new-onset cardiomyopathy diagnosis. AF-CM Group, group with cardiomyopathy with atrial fibrillation; CHF, congestive heart failure; CM, cardiomyopathy without atrial fibrillation.
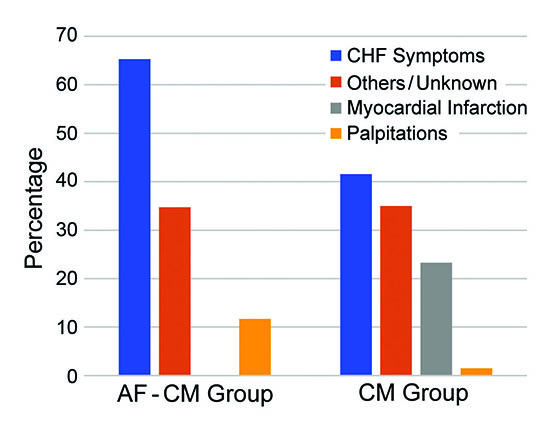
The CM group patients presented more frequently with acute CHF symptoms (41.6%) or acute myocardial infarction (23.3%). Presentation with insidious onset of CHF, was less frequent in the CM group.
A significant number of patients in both groups had varied presentations that could not be clearly related to a cardiac etiology, e.g., fall, tiredness, “not feeling right,” infection, confusion. They were grouped in the “Others/Unknown” category.
Patients in the AF-CM group were more likely to be diagnosed as outpatients than patients in the CM group (35.7% vs. 10.2%, respectively; P<0.0001); CM group patients were predominantly diagnosed in the hospital setting.
Differences in Laboratory Values and EKG
Patients with AF-CM presented with lower peak troponin values and brain natriuretic peptide (BNP) levels. Low voltage on surface EKG was more prevalent in the AF-CM group than the CM group (39.0% vs. 27.6%, respectively; P=0.0003) [Table 2].
Table 2. Electrocardiography and laboratory characteristics.
| Characteristic |
AF-CM group (n=196) |
CM group(n=197) |
P value |
| Bundle Branch Block |
|
|
0.98 |
| None |
153 (78.1) |
152 (77.2) |
|
| Left |
24 (12.2) |
25 (12.7) |
|
| Right |
19 (9.7) |
20 (10.1) |
|
| Ventricular rate |
109±26.43 |
89.7±18.80 |
<0.001 |
| BPM |
|
|
|
| Voltage group |
|
|
<0.001 |
| Low |
79 (39.0) |
54 (27.6) |
|
| High |
5 (2.5) |
24 (12.2) |
|
| Voltage (mV) |
1.8±0.85 |
2.14±1.07 |
<0.001 |
| Troponin I |
0.91±5.72 |
14.27±63.48 |
0.01 |
| BNP |
771.3 ±809.3 |
1015.6±1040.2 |
0.02 |
Data presented as n (%) or mean±standard deviation.
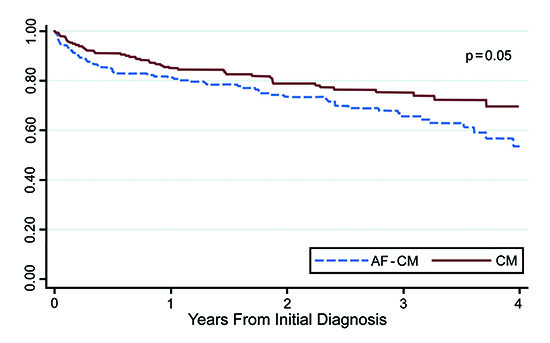
Hospital readmissions did not differ between patients with AF-CM and CM, though the mortality rate was significantly higher in patients with AF-CM and the survival curves continued to diverge throughout the follow-up data collection period [Figure 4].
Figure 4. Kaplan-Meier survival estimates. This figure represents survival of patients in cardiomyopathy with atrial fibrillation (AF-CM) and cardiomyopathy without atrial fibrillation (CM) groups.
Real-world Treatment for AF-CM Group
A large proportion of AF-CM patients (n=107, 54.6%) never saw a cardiac electrophysiologist either as an inpatient or outpatient. A majority of the patients in both groups were evaluated and treated by a cardiologist. Direct current cardioversion (DCCV) was performed only in 47 (24%) patients. Using DCCV as a surrogate for an attempt at rhythm control, only a minority of patients underwent a rhythm control strategy. Interestingly, within the AF-CM group, more patients (79 [40.3%]) underwent a diagnostic cardiac catheterization than a cardioversion procedure (24%), though none had presented with an acute myocardial infarction.
Ablation for AF was performed in a small minority (17/196 [8.7%]) of patients [Table 3]. All patients did undergo pulmonary vein isolation. Additional ablation was at the discretion of the treating electrophysiologist. The small number of patients undergoing an AF ablation procedure is especially relevant as multiple trials have demonstrated a benefit for patients who have a dual diagnosis of AF and heart failure with reduced ejection fraction. Older individuals, women, and those with a history of coronary artery disease were less likely to undergo a rhythm control strategy with either cardioversion or an ablation procedure. Those who did undergo cardioversion improved their left ventricular EF more than those who did not, and those who underwent an ablation procedure improved their EF the most. The incidence of mortality on follow-up was extremely high (40.2%) in patients who did not undergo a cardioversion or ablation, significantly lower (17%) in those who underwent a cardioversion, and markedly lower (5.9%) in those who did undergo an AF ablation procedure. This is observational data and should be interpreted with caution as there were significant confounding differences in the treatment groups [Table 4].
Table 3. Real-world treatment characteristics.
| Characteristic |
AF-CM group (n=196) |
CM group (n=197) |
| Cardiology consult |
178 (90.8) |
188 (95.4) |
| Electrophysiology consult |
89 (45.4) |
63 (32) |
| Diagnostic cardiac catheterization |
79 (40.3) |
139 (70.6) |
| Percutaneous coronary intervention |
18 (9.2) |
53 (27) |
| Direct current cardioversion |
47 (24) |
NA |
| AF ablation |
17 (8.7) |
NA |
Data presented as n (%).
Inpatient Vs. Outpatient Diagnosis
It appears that AF-CM patients have several distinctive characteristics compared to those with new-onset CM not associated with AF. To the best of our knowledge, these two groups that are commonly encountered in clinical practice have not been compared in the literature. AF-CM patients appear to have a higher likelihood of detection as an outpatient. This may be owing to the slow, insidious progression of vague symptoms like tiredness, fatigue, exertional shortness of breath, and inconspicuous weight gain. As patients in the AF-CM group are older and sicker, their sub-acute CHF or atypical symptoms are more likely to be attributed to old age or other comorbid conditions. Patients in the CM group were much more likely to be diagnosed in the inpatient setting, possibly because their symptoms had a more sudden onset as they had a higher likelihood of presenting with an acute myocardial infarction or acute symptoms of heart failure.
Typical Vs. Atypical Symptoms
A majority of patients with AF-CM did not have typical symptoms of AF (e.g., palpitations). Only 11.7% of patients were listed as having palpitations as one of their complaints. There is some evidence that atypical symptoms of AF (tiredness, fatigue, heart failure) may be associated with a more sinister form of AF 3,4. Not having the typical symptom of palpitations has also been shown to be associated with a longer duration of preceding AF and with older age 2,6. In a population-based study, palpitations were reported only by 10.35% of patients >75 years of age 7. The reason for asymptomatic or atypical symptoms in AF is unknown. There is some evidence that neuronal innervation as evaluated by I-MIBG iodine-123 (meta-iodobenzylguanidine) 8 is decreased in patients with left ventricular systolic dysfunction and may carry a worse prognosis. Furthermore, the perception of typical symptoms of AF is decreased after an AF ablation procedure 9. Is it possible that damaged or decreased cardio-neural innervation in the AF-CM group leads to a decreased perception of typical symptoms of palpitations while increasing the prevalence of atypical symptoms?
Males constituted a higher percentage of the AF-CM group (63.3% men), whereas males and females were almost equally represented in the isolated CM group (49.2% men). Men have been reported to develop AF almost a decade earlier than women 10. Several studies have also shown that “asymptomatic” AF is more common among males 1-4. The earlier development of AF with a lack of overt symptoms may predispose men to accrual of subclinical damage over time with eventual presentation as new-onset CM. Further studies are required to investigate this interesting correlation.
Voltage on surface EKG was lower in the AF-CM group than the CM group. Low voltage on surface EKG has been associated with a worse prognosis both in patients with left ventricular systolic dysfunction and in patients free of cardiovascular disease 11,12. In the AF-CM group, lower voltage may be caused by myocardial scar tissue as this group had a higher incidence of coronary artery disease, higher body mass index, or unknown factors.
Differences in Cardiac Biomarkers
Higher troponin levels have been found to be an adverse prognostic marker in heart failure and a wide variety of cardiovascular diseases 13,14. In our study, peak troponin levels were lower in patients with AF-CM than in patients with isolated CM, but, paradoxically, the mortality for the AF-CM group was higher. One of the reasons for lower levels of troponin in the AF-CM group compared to the CM group may be that the latter more commonly had acute myocardial infarction as the presenting complaint. BNP has also been associated with diagnosis of heart failure 15 and as a prognostic factor, with higher levels portending a worse prognosis 16. However, BNP levels were also lower in AF-CM patients, despite them presenting more often with CHF symptoms. This may be owing to a slower progression of symptoms in the AF-CM group or to a slightly higher body mass index in AF-CM patients as obesity also has been found to attenuate BNP levels 17. Interestingly, despite lower troponin and BNP levels, which usually confers better prognosis, mortality was significantly higher in the AF-CM group.
Differences in Hospital Readmissions and Mortality
Hospital readmissions were no different between the two groups, though mortality was significantly higher in the AF-CM group. As shown in [Figure 4], the mortality curves were still diverging after almost 4 years of follow-up. Our reviewed data revealed low utilization of electrophysiologic expertise, cardioversions, or ablation strategy in the management of patients with AF-CM.
Differences in Patient Management
Some recent studies have found a lower risk of death and other cardiovascular complications associated with specialist care in AF 18,19. There is also some evidence that heart failure patients treated by cardiologists have better outcomes than patients treated by general practitioners 20,21. There are limited data about what percentage of patients with AF-CM in the real world are evaluated by a cardiac electrophysiologist or undergo an ablation procedure. This is especially relevant as more evidence is accumulating that an ablation strategy may be beneficial for patients with left ventricular systolic dysfunction and AF 22-25.
Our sample is representative of the practice in the Aurora Health Care system, a large health care system in the Midwest. This may or may not reflect either Midwestern or national patterns. A large proportion of patients in the AF-CM group (n=107 [54.6%]) were never evaluated by a cardiac electrophysiologist, and for most of these patients, no cardioversion or ablation was performed (n=132 [67.3%]). A minority of patients underwent an ablation procedure (17/196 [8.7%]). There appeared to be significant bias in patients who were referred for a rhythm control strategy. Older patients, those with a history of coronary artery disease, and women were less likely to receive either a cardioversion or an ablation procedure. With a history of coronary artery disease, there may be a perception that CM is ischemic and conversion to sinus rhythm would not be helpful. Whether that perception is true is unclear. The lower likelihood of older patients and women receiving these interventions may reflect a systemic bias. These factors need to be evaluated further in larger population studies.
Those who did undergo a rhythm control strategy showed significant improvements in their left ventricular EFs, with the most robust response observed in those undergoing an ablation procedure [Table 4]. Patients who underwent these procedures had markedly low mortality on follow-up compared to the no-intervention cohort, though there were significant confounding factors between these groups that make causal inferences inappropriate.
Table 4. Patient comparison with and without rhythm control intervention within AF-CM group.
| Characteristic |
No intervention n=132 |
DCCV n=47 |
DCCV + ablation n=17 |
P value |
| Sex |
|
|
|
0.02 |
| Female |
57 (43.2%) |
12 (25.5%) |
3 (17.6%) |
|
| Male |
75 (56.8%) |
35 (74.5%) |
14 (82.4%) |
|
| Age, years |
77.61±11.34 |
66.15±9.34 |
62.06±7.32 |
<0.001 |
| Ethnicity |
|
|
|
0.78 |
| Hispanic/Latino |
1 (0.8%) |
0 (0.0%) |
0 (0.0%) |
|
| Not Hispanic/Latino |
131 (99.2%) |
47 (100.0%) |
17 (100.0%) |
|
| Tobacco use |
78 (59.1%) |
30 (63.8%) |
11 (64.7%) |
0.8 |
| Hypertension |
96 (72.7%) |
32 (68.1%) |
10 (58.8%) |
0.46 |
| Diabetes mellitus |
44 (33.3%) |
12 (25.5%) |
3 (17.6%) |
0.3 |
| Coronary artery disease |
56 (42.4%) |
6 (12.8%) |
4 (23.5%) |
<0.001 |
| Death |
53 (40.2%) |
8 (17.0%) |
1 (5.9%) |
<0.001 |
| Baseline LVEF, % |
29.62±7.85 |
29.81±7.54 |
28.18±6.94 |
0.74 |
| Follow-up LVEF, % |
44.66±12.42 |
50.46±11.49 |
56.71±6.89 |
<0.001 |
Data presented as n (%) or mean±standard deviation.
Each patient chart was thoroughly evaluated by a research coordinator to identify a group of new-onset CM patients with a concomitant or antecedent diagnosis of AF (AF-CM group); the CM group patients were also carefully assessed to rule out any contribution of dysrhythmias to CM. Nonetheless, it is possible that some CM group patients had AF that was undiagnosed or not captured in medical documentation or EKG, telemetry, or rhythm strip evaluation. We excluded patients with a cardiovascular implantable electronic device because a significant percentage of them have pre-existing structural heart disease, and also, pacing can confound both patient characteristics and outcomes. Thus, we obtained as uncontaminated a sample as possible so that patients with AF-CM and CM without any dysrhythmias could be compared. But this is a retrospective study with all the limitations inherent in that type of study, including incomplete or inaccurate data and the possibility of selection bias. Echocardiographic reports were utilized for assessing left ventricular EF; sometimes, these can be challenging to read, especially in patients with atrial dysrhythmias. One of the reasons a cut-off of 40% was selected was to minimize the probability of patients with a normal EF being included in the study.
Patients in whom AF either precedes or is concomitant with development of new-onset CM (defined as left ventricular EF ≤40%), appear to have significant differences compared to patients who develop CM without AF. In our study, the AF-CM group was older and more likely to be male; had more comorbidities, lower voltage on surface EKG, and lower cardiac biomarkers; and seemed to have more insidious onset of symptoms but still a significantly worse prognosis. We hypothesize that AF-CM represents a specific type of cardiomyopathy with a distinctive etiology, presentation, and outcomes. Only a small percentage of patients in the AF-CM group underwent cardioversion and a smaller percentage yet underwent an ablation procedure, but those who did fared remarkably better than those who did not receive these interventions. Women, those with a history of coronary artery disease, and older patients were less likely to undergo these interventions. Whether this reflects a systemic bias in referral and treatment needs to be investigated further with larger, population-based studies.
The authors are grateful to the Aurora Research Institute for its support, Jennifer Pfaff and Susan Nord of Aurora Cardiovascular and Thoracic Services for editorial preparation of the manuscript, and Brian Miller and Brian Schurrer of Aurora Cardiovascular and Thoracic Services for assistance with the figures. Special thanks to Dr. Roderick Tung at the University of Chicago for his suggestions and input, and the Aurora BayCare Medical Center research interns for data acquisition.






