The story of a Migrating Pericardial Drain and Perforation!
Mehmet Ali Elbey1, Rakesh Gopinnathanair1, Dhanunjaya Lakkireddy1
1Kansas City Heart Rhythm Institute (KCHRI), Overland Park, Kansas.
A patient underwent the LARIAT left atrial appendage (LAA) ligation procedurewith persistent atrial fibrillation history. The procedure was done successfully. A transthoracic echocardiography did not show pericardial effusion. The patient was examined under fluoroscopy where the tip of the drain was not in the pericardial space and contrast injection pericardial drain confirmed its location in the inferior vena cava.
Key Words : .
Dhanunjaya Lakkireddy, MD, FACC, FHRS
Executive Medical Director
The Kansas City Heart Rhythm Institute (KCHRI) @ HCA MidWest
Professor of Medicine, the University of Missouri - Columbia
12200, W 106th street, Overland Park Regional Medical Center
Overland Park, KS 66215
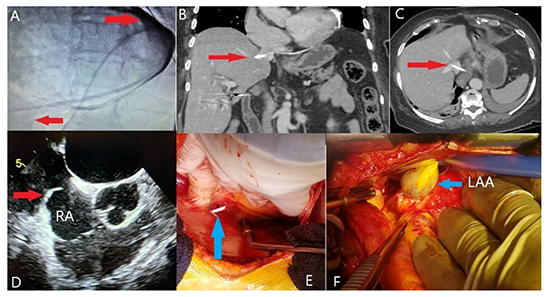
An 80-year-old woman with a history of persistent atrial fibrillation underwent the LARIAT left atrial appendage (LAA) ligation procedure. The procedure was uneventful and at the end a straight pericardial drain (Boston Scientific, Marlborough, MA, USA) was placed to allow further evacuation of the space from the ligated LAA. The patient did well for the first 18 hours with no further drainage. The next day morning patient complained of significant chest pain and many bouts of deep coughing. Immediately after that the patient’s pericardial drain starting putting out a significant amount of dark venous blood suggestive of possible recurrent pericardial effusion. A transthoracic echocardiography did not reveal any pericardial fluid. The patient was examined under fluoroscopy where the tip of the drain was not clearly visible in the pericardial space. Contrast injection through pericardial drain confirmed its location in the hepatic vein-inferior vena cava (IVC) confluence. (Panel A, arrows). Computed tomography (CT) also was performed and identified that the pericardial drain has migrated into the IVC and the tip was in the middle hepatic vein (Panel B-C, arrows). This confirmed the migration of the pericardial drain tip from the pericardial space into the IVC. Further review of the echocardiography and CT confirmed a very thin area of tissue at the junction of the IVC and right atrium (RA). It is likely that this vulnerable area was punctured due to patient movement and violent bouts of coughing. The location of the drain was confirmed and repaired under direct visualization in the operating room transesophageal echocardiography was performed and confirmed the catheter to be in the IVC, piercing it right at the atrial junction (Panel D, arrow). Median sternotomy was performed and established aortic and right atrial appendage cannulation. It should be noted that the catheter was still in the right atrial and the IVC junction (Panel E, arrow). The catheter was pulled, and the hole was closed with a suture with no residual bleeding. A full maze procedure was also done. There was a LARIAT suture noted on the left atrial appendage that was excluding a large part of it (Panel F, arrow). The patient tolerated the procedure well, then she was discharged in stable condition.
It is important to realize vulnerable anatomy and make sure that the catheter tip doesn’t migrate towards the great vessels. It is preferred to avoid a straight tipped pericardial drain and care must be taken to ensure the location of the tip away from the inferior or superior vena cava.
Figure 1. The distal part of catheter shows contrastin the vena cava inferior with Fluoroscopy (Figure-A, arrows) and the catheter was demonstrated with CT (Figure-B and C, arrows) and transesophageal Echocardiography (Figure-D, arrow) in the right atrium and inferior vena cava junction. Intraoperative images show the catheter (Figure-E, arrow) and excluded left atrial appendage (Figure-F, arrow)