Management of the Asymptomatic Patient After
Catheter Ablation of Atrial Fibrillation
David S. Frankel, M.D., Edward P. Gerstenfeld, M.D.
From the Section of Cardiac Electrophysiology, Division of Cardiology, Department of Medicine, Hospital of the University of Pennsylvania, Philadelphia, PA.
Ablative therapy for atrial fibrillation is becoming more commonplace, and some minimally symptomatic or asymptomatic patients will be referred for ablative therapy. Reasons to ablate asymptomatic patients include young age and/or the presence of a tachycardia induced cardiomyopathy; in addition, some symptomatic patients may become asymptomatic after ablation. Managing these patients can be challenging. In this review, we will discuss the use of telemetric monitoring, antiarrhythmic drugs and anticoagulation after ablation in asymptomatic patients with atrial fibrillation.
Correspondence to: Edward P Gerstenfeld MD, 9 Founders Pavilion, 3400 Spruce Street, Philadelphia PA 19104.
Ablation of atrial fibrillation (AF) has been gaining popularity since it was initially described by Haissaguerre and colleagues in 1998.1 While initially reserved for patients with structurally normal hearts and extremely symptomatic AF refractory to multiple antiarrhythmic drugs (AAD), the indications for ablation have continued to broaden. According to the recently published guidelines for the management of AF by the American College of Cardiology, American Heart Association and European Society of Cardiology, catheter ablation is now considered standard of care after a patient has developed recurrent AF on one AAD.2 Wazni and colleagues demonstrated that in patients with new onset AF, the outcome at one year with AF ablation was superior to treatment with AAD.3 Hsu and colleagues, as well as our laboratory, have demonstrated that the outcome of AF ablation in patients with heart failure and left ventricular dysfunction is reasonable and typically leads to improvement in left ventricular function.4,5
Yet, one may reasonably wonder why AF ablation should ever be performed in the asymptomatic patient. The AFFIRM study found no mortality benefit to maintenance of sinus rhythm with AAD(s) compared to a strategy of ventricular rate control and anticoagulation.6 Studies using prolonged external monitoring after AF ablation have found a significant incidence of asymptomatic AF after ablation, and recent studies have shown that late recurrences of AF can continue to occur even five years after the initial ablation procedure.7-9 The guidelines state that discontinuation of warfarin should be based on the patients CHADS2 score rather than freedom from AF recurrence.2,10 Importantly, two recent multicenter reviews from Cappato and colleagues have described a 6% incidence of major complications from AF ablation, including a 1/1000 risk of death.11,12 So, what is the potential benefit of AF ablation in the asymptomatic patient?
For this review, we will limit our discussion to the truly asymptomatic patient. Patients with unclear symptoms who realize they feel better only after conversion to sinus rhythm are not uncommon, and are not the population presently considered. In our opinion, there are several reasons to consider AF ablation in the asymptomatic patient. The first is to achieve a potentially underestimated, long term mortality benefit in young patients with AF. The AFFIRM trial compared strategies of rate and rhythm control in patients who were either older than age 65 or had other risk factors for stroke or death.6 The mean follow-up of 3.5 years is certainly reasonable for a prospective, multicenter, randomized trial, but hardly reflects the long-term outlook of a 35 year old with AF who has decades of life ahead. The rhythm control strategy in AFFIRM predominantly utilized AAD rather than ablation to maintain sinus rhythm. Many AAD have side effects and may in fact increase mortality.13,14 Although patients in AFFIRM were randomized to rate or rhythm control “strategies,” only 2/3 of patients randomized to the rhythm control strategy remained in sinus rhythm at the end of the study, compared to 1/3 of patients in the rate control arm.6 In a post-hoc analysis of AFFIRM, patients who actually achieved and maintained sinus rhythm were compared to those who remained in AF.15 There was a nearly two fold higher mortality among patients who were in AF at the end of the study, and the predictors of increased mortality included the use of AAD. The authors conclude that, “if an effective method for maintaining sinus rhythm with fewer adverse effects were available, it might improve survival.” Therefore, in a young patient with AF and few comorbidities, there is some evidence that restoring sinus rhythm may improve long term survival. In addition, restoration of sinus rhythm prevents the long term atrial dilatation and adverse electrical and mechanical remodeling that can occur with AF.16,17 Further, the potential long term risk of major bleeding (2.2 events per 100 patient-years) from anticoagulation with warfarin remains.18 The CABANA trial is prospectively investigating the long term effect on mortality of catheter ablation compared to medical therapy.19
A second reason to ablate asymptomatic AF is to reverse a tachycardia-induced cardiomyopathy. While the onset of this condition is typically gradual, recurrent tachycardia in a patient with a prior tachycardia-mediated cardiomyopathy can lead to a precipitous decline in cardiac function, with development of heart failure and even death.20 Hsu and colleagues reported a 21% improvement in left ventricular ejection fraction (LVEF) following catheter ablation in patients with AF, heart failure and LVEF<45%.4 Gentlesk and colleagues from our laboratory reported similar improvement in LVEF following ablation, even among cardiomyopathy patients with apparent ventricular rate control in AF prior to ablation.5 Thus, it is reasonable to consider AF ablation to reverse a cardiomyopathy caused by AF, and to prevent recurrent cardiomyopathy in a patient in whom a prior tachycardia–mediated cardiomyopathy occurred.
Finally, management of asymptomatic AF is important because some patients who have symptomatic AF prior to ablation may become asymptomatic after ablation. For example, in a study by Hindricks and colleagues, AF ablation was performed in patients with highly symptomatic AF.7 In the seven day Holter recordings prior to ablation, only 5% had exclusively asymptomatic AF. When seven day Holter monitors were repeated six months following ablation, 37% had exclusively asymptomatic episodes. The mechanism whereby symptomatic AF becomes asymptomatic after ablation is unclear, but may involve modification of the autonomic nervous system with ablation. While this highlights the importance of monitoring for asymptomatic AF, it also emphasizes that dealing with patients with asymptomatic AF following ablation is not uncommon.
Multiple studies have documented that patients frequently have asymptomatic AF following ablation;7,9 therefore, monitoring for recurrence should not rely on symptoms alone. Many patients undergoing ablation also have a heightened awareness of palpitations and may report symptoms of palpitations from atrial or ventricular premature beats rather than AF. Because the presence of recurrent AF has important implications for continued anticoagulation and antiarrhythmic treatment, objective telemetric monitoring of the heart rhythm is of paramount importance. It also should be recognized that patient compliance with home monitoring is greatest soon after the ablation procedure, and decreases with time.
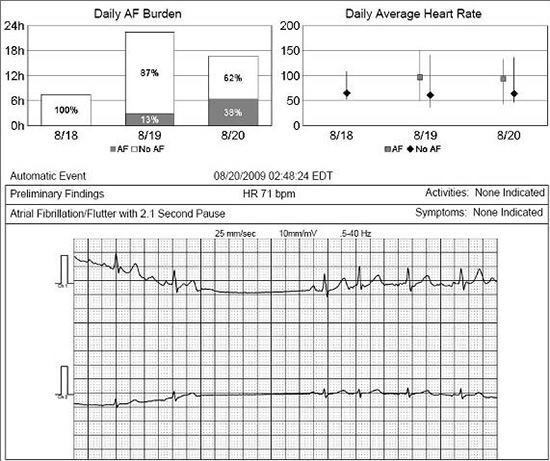
Our practice is to demonstrate use of a transtelephonic monitor (TTM) to all patients in the hospital the day after ablation, and then to send patients home with a 30-day monitor with either continuous monitoring capability or an auto-trigger algorithm to detect asymptomatic AF in addition to symptomatic, patient triggered episodes Figure 1. Patients are also instructed to transmit a strip of their heart rhythm twice daily regardless of symptoms. The monitor aids in the detection of AF even during the typical 6 to 8 week “blanking period” following ablation. In patients with recurrent AF after ablation, the TTM can confirm patient symptoms, aid in the adjustment of antiarrhythmic and AV nodal blocking medications, and guide the scheduling of cardioversions. There is evidence that in patients with paroxysmal AF, early AF recurrence suggest a significantly increased risk of late AF recurrence, and therefore a lower likelihood of complete AF cure.21,22 We perform a second 30-day monitor at 6-months after ablation or whenever the discontinuation of warfarin is considered in patients with CHADS2 risk factors for stroke. Additional monitors are sent to patients if any symptoms of recurrent AF occur outside of these windows.
Figure 1. Information recorded from transtelephonic monitor in a patient who underwent atrial fibrillation (AF) ablation. The top panel indicates the percentage of each day spent in sinus rhythm vs. atrial fibrillation according to the monitor, as well as the mean ventricular rate in AF compared to sinus rhythm. A sample rhythm strip is provided in the bottom panel, during which AF terminates, followed by a single sinus beat and then reinitiation of AF. This episode was asymptomatic
Post Ablation Antiarrhythmic Therapy
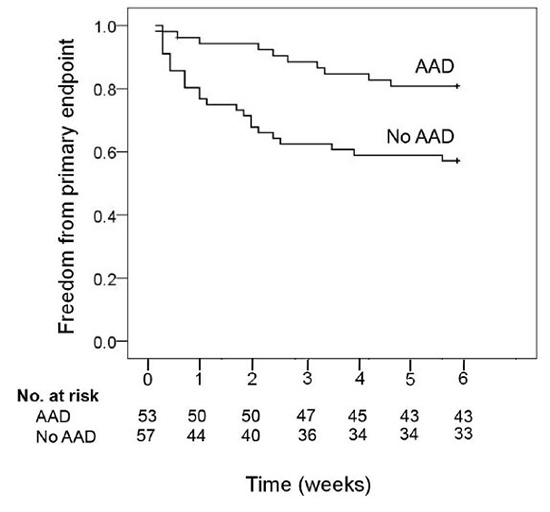
Most patients undergoing ablation have tried an AAD prior to the ablation procedure. The practice after ablation varies by institution and practitioner. Many physicians choose to continue antiarrhythmic therapy for 6-weeks after ablation in paroxysmal AF patients to facilitate the reverse atrial remodeling that occurs in sinus rhythm and to limit the inconvenience of recurrent AF in the early period. Others send patients home without AAD, with a plan to resume them if AF recurs. In order to test the hypothesis that antiarrhythmic therapy after ablation reduces the need for recurrent hospitalization or cardioversion after ablation, we randomized 110 patients with paroxysmal AF to six weeks of AAD therapy plus AV nodal blocking agents versus AV nodal blocking agents alone immediately following AF ablation.23 The primary endpoint was a composite of clinically significant atrial arrhythmias lasting over 24 hours or requiring initiation of AAD therapy, cardioversion or hospital admission, or intolerance to an AAD requiring drug cessation. The composite endpoint was significantly reduced in the AAD compared to the no-AAD arm [19 vs. 42%; p=0.005, Figure 2]. Including only the hard endpoints of recurrent arrhythmia lasting > 24 hours and need for cardioversion or hospital ization, there remained a significant reduction in the AAD group (13 vs. 28%; p=0.05). Therefore, it is our practice to continue AAD in all patients with paroxysmal AF for 6 weeks following ablation. As most patients have been on an AAD in the past, we typically resume a previously tolerated AAD and AV nodal blockade the evening after ablation; patients can then be discharged the following day without the need for extensive inpatient monitoring. Patients are seen in the office at 6-weeks following ablation and the drug is discontinued in patients with no recurrent AF. In those with frequent recurrent episodes of AF, the AAD is continued and the patient is reevaluated at 6 months.
Figure 2. In the 5A study, patients who were treated with antiarrhythmic drugs (AAD) for six weeks following atrial fibrillation ablation had a lower incidence of the primary endpoint than those treated with just AV nodal blocking agents. The primary endpoint was a composite of atrial arrhythmias lasting more than 24 hours; atrial arrhythmias associated with severe symptoms requiring hospital admission, cardioversion, or initiation/change of antiarrhythmic drug therapy; and intolerance to antiarrhythmic agent requiring drug cessation. (From Roux JF et al. Circulation 2009;120:1036-1040)
For patients with persistent AF, most electrophysiologists would continue the AAD after ablation to promote sinus rhythm and thereby facilitate reverse electrical and mechanical remodeling, as well as to decrease the need for early cardioversion. We typically continue antiarrhythmic agentsfor six months following ablation in persistent AF patients, after which the drug is discontinued for those patients maintaining sinus rhythm.
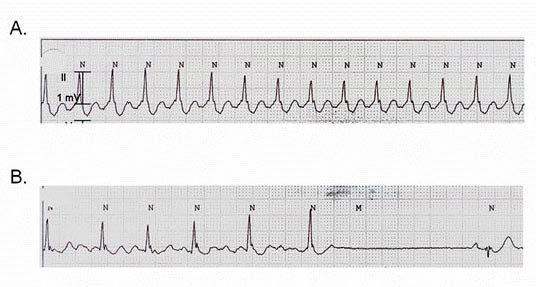
Occasionally, patients can develop a rapid organized atrial tachycardia following ablation. While the initial strategy for management of these troublesome tachycardias includes cardioversion and use of an AAD, we have found that class IC drugs which block sodium channels and facilitate slow conduction can occasionally perpetuate these arrhythmias Figure 3. A trial of AAD cessation can be helpful in these patients prior to considering repeat ablation.24
Figure 3. A telemetry strip recorded from a patient who developed an organized atrial tachycardia while being treated with flecainide following catheter ablation of atrial fibrillation. Flecainide was discontinued when the patient was admitted to the hospital the night before a scheduled repeat ablation procedure. During the evening, the atrial tachycardia degenerated into atrial fibrillation and then converted to sinus rhythm. We hypothesize that in some cases, slow conduction facilitated by Class IC agents may facilitate organized atrial tachycardias after ablation. We have found that on occasion, a trial of antiarrhythmic drug cessation can result in termination of these organized tachycardias
Post Ablation Anticoagulation
Discontinuation of warfarin remains the most controversial decision following AF ablation. According to the guidelines written by the American College of Cardiology, American Heart Association and European Society of Cardiology, long term anticoagulation for stroke prevention should be recommended for those with AF and CHADS2 risk scores of 2 or greater unless contraindications are present. Warfarin should be considered for those with a score of 1 and should not be reco mmended for those with a score of 0. Aspirin is an alternative to warfarin in patients at low risk (CHADS2≤1) or in those with contraindications to warfarin.2 While these guidelines suggest that warfarin therapy following ablation should be based on the CHADS2 score and not the presence or absence of AF, most patients are extremely motivated to discontinue warfarin, and instructing patients to continue warfarin when no detectable AF is present can be challenging. Furthermore, anticoagulation with warfarin increases the risk of intracranial hemorrhage two to five-fold.22,25 However, as documented by Shah and colleagues, late AF recurrences can occur, even after several years of apparent freedom from AF following ablation.9 Thus, the optimal anticoagulation strategy following AF ablation needs to be tailored to the individual risks and preferences of the patient. Three series have examined the safety of discontinuing warfarin following AF ablation. Oral and colleagues studied 755 patients with paroxysmal (490) or chronic (265) AF. Fifty-six percent had CHADS2 risk scores of 1 or greater.26 AAD were discontinued two to three months following ablation. All participants were anticoagulated with warfarin for three months following ablation, and then warfarin was discontinued in patients without symptomatic AF recurrences. Some thromboembolic events occurred early after ablation despite warfarin use, most (7 of 9) in the first two weeks. Of the 522 patients who remained in sinus rhythm during the first three months, aspirin was substituted for warfarin in 79% of those with a CHADS2 risk score of 0 and 68% of those with CHADS2 risk scores of 1 or greater. None of these patients developed a thromboembolic event during mean follow-up of 25 months.
We followed 1,058 patients who underwent AF ablation at our institution between 1999 and 2005.27 Guidelines for the discontinuation of warfarin after ablation included a left atrial size <4.5cm, CHADS2 score of 2 or less, no prior stroke or TIA, and the absence of AF on two 30- day TTMs over a 6-month period. Warfarin was eventually discontinued in 31% of patients. Over a mean follow-up of 3.5 years, only one patient (0.3%) had an embolic stroke off warfarin; this patient was later documented to have recurrent AF.
Finally, the experiences of four centers, including our own, were combined into a large series of 2,436 patients undergoing AF ablation who discontinued warfarin.28 Sixty-five percent had paroxysmal AF, 16% persistent AF and 19% “permanent” AF. CHADS2 risk score was 0 in 62%, 1 in 27% and 2 or greater in 11%. Warfarin was discontinued in 2,436 patients after ablation. During a mean followup of 31 months, only one patient had a stroke (0.04%). Therefore, discontinuation of warfarin is feasible in the appropriate patient with a good short term outcome. Longer term followup will be required to confirm these findings.
We recommend discharging all patients after ablation with a 7 to 30-day TTM with instructions to transmit strips twice daily and with any symptoms. A monitor with continuous telemetry or an algorithm for automatic AF detection should be used to assure detection of asymptomatic AF. Delivery of the monitor directly to the patient after ablation allows demonstration of proper use at a time when compliance with TTM use is highest. A second 7 to 30 day TTM should be used outside the “blanking period” to detect asymptomatic AF and determine procedure efficacy. Additional monitors may be sent to patients with symptomatic palpitations that cannot be easily documented with an ECG.
Post Ablation Antiarrhythmic Therapy
Based on the results of the 5A study, we discharge all patients with paroxysmal AF who have previously used an AAD on the previously tolerated AAD to reduce the need for early cardioversion and hospitalization.23 Antiarrhythmic therapy is continued for 6 weeks. Therapy of patients with no prior AAD use is individualized. All patients with persistent AF are also discharged on AAD which is typically continued for 6 months.
Post Ablation Anticoagulation with Warfarin
In conjunction with the consensus statement from the Heart Rhythm Society, European Heart Rhythm Association and European Cardiac Arrhythmia Society, all patients are discharged after ablation on warfarin anticoagulation.29 While one study has suggested that aspirin may suffice in low risk patients, the risk of thromboembolism after ablation warrants warfarin use, in our opinion.30 Patients are either continued on warfarin through the ab lation procedure, or bridged with heparin or lovenox immediately following ablation. In patients with CHADS2 risk scores of 0, there is no indication for long term warfarin even if AF recurs; therefore we discontinue warfarin in favor of aspirin 325 mg daily at 6 weeks. This group comprises a significant proportion of patients undergoing AF ablation.27 Patients with CHADS2 scores of 1 have the option of aspirin or warfarin therapy according to American College of Cardiology, American Heart Association and European Society of Cardiology guidelines. We give CHADS2 1 patients with no symptoms of recurrent AF and no asymptomatic AF detected on two TTMs the option of discontinuing warfarin at 6 months. The treatment of CHADS2 2 patients is controversial. In CHADS2 patients at lower risk of stroke (no history of stroke or transient ischemic attack (TIA), left atrial size <4.5 cm, normal left ventricular function), if there are no symptoms of recurrent AF for six months after ablation with confirmation on two 30-day auto-trigger TTMs, the option of warfarin cessation is discussed with the patient after reviewing the risks and benefits. Some patients may elect to continue on long term warfarin therapy. The option of warfarin cessation is based on the results of the three studies reviewed above, demonstrating a low risk of thromboembolic events in selected patients and the established bleeding risk with continued warfarin therapy.25-28 All patients are instructed to take their pulse twice daily for the rest of their lives and report any palpitations or symptoms of AF. Patients with a prior stroke or TIA, left atrial dilatation, left ventricular dysfunction or a CHADS2 score of 3 or greater are advised to continue anticoagulation with warfarin indefinitely. Decisions regarding warfarin cessation in higher risk patients after long term follow-up can be individualized.






