A 60-year-old male was seen in the office for follow-up after a recent diagnosis of cardiac sarcoidosis. He was treated with Infliximab and Mycophenolate Mofetil. He was confirmed to be responding to immunosuppressive therapy on a recent PET scan. Several months before his visit, he began developing elliptical-shaped areas of erythema on his posterior and lateral aspect of his right/left (?) lower extremity. The erythema progressed with development of central eschars followed by ulcerations ascending proximally up his leg [Figure 1]..
We started treatment for Nocardiosis prior to biopsy because my attending visually diagnosed the condition prior to biopsy as he had seen it before when on rotation as a medical student at an infectious disease hospital in India. After a provisional diagnosis of Cutaneous Nocardiosis, and he was then started on 8-12 weeks of Trimethoprim-Sulfamethoxazole (5-10 mg/kg/day) which was later confirmed on biopsy.
Figure 1. Temporal Progression (earliest: top left, most recent: bottom right) of Cutaneous Nocardiosis

After clinical improvement was noted several weeks later, the patient was restarted on his immunosuppressive therapy. He was initially treated with oral corticosteroids for 6 months. After a repeat scan, it was determined that longer courses were needed, so infliximab (3 mg/kg) was added.
Several weeks followed before he noticed fatigue, malaise, and a maculopapular, non-pruritic rash on his lower extremity [Figure 2] that preceded the development of fever prompting hospitalization for 3 days. Symptoms temporarily improved after treatment with broad-spectrum antibiotics during this time with the resolution of the rash. However, shortly after discharge, he began spiking high fever with temperature reported at 1040F, prompting re-hospitalization. After the initial workup was found inconclusive, the patient was transferred to a local tertiary center as he began to worsen clinically. Upon transfer, he was admitted to the intensive care unit for septic shock secondary to Histoplasmosis. Histoplasmosis was diagnosed with Enzyme immunoassay (ELISA) by Histoplasma antigen detection in serum and urine. Aggressive management with systemic antimicrobial therapy [Amphotericin deoxycholate (07-1 mg/kg/d), Vancomycin (500 mg every 6hrs) and Piperacillin & Tazobactam (4.5g every 8h)], volume resuscitation and vasopressors resulted in significant clinical improvement over five days with an unremarkable subsequent clinical course. After discharge, the patient completed treatment with amphotericin B before follow-up in the clinic. At the time of presentation, he additionally reported a painful clustered vesicular rash with an erythematous base on his lateral side of his leg, which recently developed. By observation, it appeared to have grouped vesicles consistent with Herpes simplex, for which the patient was treated with Valacyclovir (1000 mg BID 7 days) [Figure 3].
Figure 2. Generalized Maculopapular Rash of Early Cutaneous Histoplasmosis.
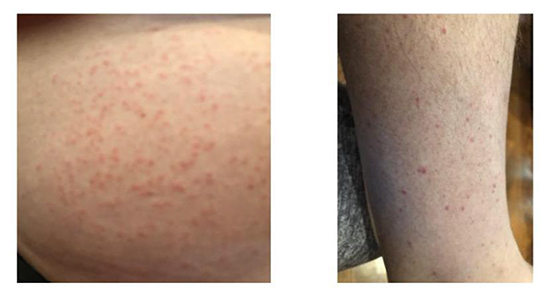
Figure 3. Clustered vesicular rash with erythematous base consistent with HSV.

Sarcoidosis is a systemic granulomatous disease characterized by non-caseating granulomas in various organs such assk in, joints, lungs, brain, and heart, which can progress to fibrosis2. The pathophysiology of sarcoidosis involves three significant events: Exposure to antigen; acquired cellular immunity directed against the antigen, and the appearance of immune effector cells which promote a non-specific inflammatory response3.
Dermatological infections can develop in 20% of immunocompromised hosts due to the breakdown of anatomical
barriers4. With different degrees of immunosuppression in sarcoidosis patients, there can be variable clinical presentations of dermatological infections. With varied clinical presentations , skin infections in sarcoidos is patients can mimic a lot of differential diagnoses such as drug rashes transfusion rashes, hemorrhagic rashes, and malignancies which should be excluded from necessary diagnostic tests5. In this regard, it is essential to keep in mind that a mild dermatological manifestation might represent a severe underlying systemic disease or malignancy5. Moreover, there might be the dissemination of infection from organs such as the lung or gastrointestinal tract to the skin due to impairment of host defenses such as neutrophil count, humoral and cellular immunity4. Alternatively, the infection can spread from a localized dermatological site to other systemic organs if there is a severe compromise in host defense mechanisms 4.
Impairment of cell-mediated immunity and corticosteroid therapy are the most important factors that can predispose to the development of opportunistic infections in sarcoidosis6, 7. Additionally, other risk factors that can lead to the development of opportunistic infections in sarcoidosis include neurological or cardiac involvement, ≥3immunosuppressive drugs (Cyclophosphamide), CD4 lymphopenia age, sex, and ethnicity 8-10. Some of the most common opportunistic infections in sarcoidosis include cryptococcosis (59%), tuberculosis (13%), nocardiosis (11%), histoplasmosis (9%), pneumocytosis (9%) and Aspergillosis (7%) 8. The acute form of nocardiosis can present as pustules, abscesses, subcutaneous nodules in sporotrichoid pattern4. Whereas, the chronic formcan present as chronic purulent ulcerating draining nodules (mycetoma’s)4. Alternatively, the dermatological infection can disseminate by blood to various organs such as the brain, kidneys, lymphatics, and pericardium to manifest as firm cutaneous or subcutaneous abscesses 4, 11. According to Jamilloux, Y. , nocardiosis in corticosteroid treated patients can present as an exacerbation of pulmonary sarcoidosis or disseminated abscesses6. Gram staining of the skin lesions demonstrates beaded, delicate, and branching filaments of nocardiosis to confirm the diagnosis4. Histopathological diagnosis of nocardiosis can also be confirmed with brown-brenn, or methenamine silver staining with the fungal presence in characteristic abscesses 4.
In patients with asevere form of sarcoidosis, corticosteroids are the usual mainstay of therapy 6. In patients who have an inadequate response or cannot tolerate glucocorticoid side effects, alternative agents such as methotrexate, infliximab, or mycophenolate mofetil are used either as a monotherapy or in combination1, 12. Anti-Tumor necrosis factor (TNF) medications like infliximab effectively inhibit granuloma formation, but can paradoxically result in sarcoid-like reaction, psoriatic skin lesions, non-melanotic skin cancers, susceptibility for invasive fungal infections, and worsening of heart failure13-15.Consequently, anti-TNF agents are not used as first-line immunosuppressive therapy for sarcoidosis. Among other alternative agents used, mycophenolate mofetil is also associated with cutaneous adverse reactions such as skin rash, ecchymoses, and cellulitis16.
Patients with cardiac sarcoidosis are often on chronic immunosuppressive therapy. Data is modest in regards to optimal dose and treatment duration, but many physicians elect to continue glucocorticoid therapy for 1-2years12. Consequently, patients are prone to develop a variety of conditions involving the skin such as sequelae of immunosuppression (infectious vs. malignancy), adverse reactions, and breakthrough disease. The differential diagnosis of skin lesions in an immunocompromised sarcoidosis patient is broad so that we will focus on the general cutaneous conditions observed:cutaneous sarcoidosis, cutaneous no cardiosis, cutaneous involvement in disseminated histoplasmosis, and herpesvirus.
Cutaneous sarcoidosis is found in approximately 25 percent of patients with sarcoidosis and can present at any stage of the disease1 They more commonly present in the African American population and women2. Manifestation is variable and can have specific (non-caseating granulomas) or non-specific (e.g., erythema nodosum) lesions. Specific manifestations of cutaneous sarcoidosis includ elupus pernio, infiltrated plaques, maculopapular lesions, subcutaneous nodules, and scars2. Studies have shown that specific lesions in conjunction with bronchoalveolar lavage (revealing lymphocytosis with high CD4/ CD8 ratio) and elevated serum Angiotensin Converting Enzyme (ACE) levels can predict progressive disease in sarcoidosis1. Cutaneous lesions, which are easily obtained via punch biopsy, and therefore have prognostic implications that can guide therapy. Systemic immunosuppression is reserved for rapidly progressive cutaneous sarcoidosis, whereas anti-TNF medications are reserved for refractory disease17.
Nocardiosis most commonly presents as pulmonary disease in immunocompromised patients, but may infrequently present as a cutaneous manifestation (8%)18. Cutaneous infections typically result from direct inoculation or as a disseminated consequence of the inhaled athogen and are clinically indistinguishable from Staphylococcus aureus and group A Streptococcus. These lesions may present as ulcerations (as in our patient), subcutaneous abscesses, pyoderma, cellulitis or nodules18, 19. Empiric monotherapy for isolated cutaneous infections includes Trimethoprim-Sulfamethoxazole (used in our patient) or minocycline, with no need for immunosuppression20. However, in severely immunocompromised patients, the usual therapy for cutaneous nocardiosis includes trimethoprim-sulfamethoxazole and antimicrobial agent (cefotaxime, imipenem, or amikacin) 4.
Cutaneous involvement in disseminated histoplasmosis is typically observed in patients with AIDS or those with profound defects in cellmediated immunity and occurs in 10 to 15 % of cases. The lesions are non-specific and highly variable in presentation, including nodular, papular, plaque-like, ulcerative, vesicular, or generalized dermatitis. In progressive disseminated disease, patients present with fever, weight loss, hepatosplenomegaly, and hematologic disturbances. If untreated, there is a 100% mortality rate21.
The physical manifestations of Herpes simplex virus (HSV) in immunocompromised patients are similar to immunocompetent hosts, but may have larger lesions, necrotizing ulcers, or involve widespread areas that are not necessarily in the perioral or genital regions. HSV infections appear as clustered vesicles on an erythematous base, which progress to a pustular or ulcerated lesion, and then form a crust before healing. Antiviral agents such as acyclovir, famciclovir, and valacyclovir are used as therapeutic and prophylactic treatment22.
A broad differential diagnosis should be considered for cutaneous lesions in an immunocompromised host, especially when the clinical picture may be obscured by a known diagnosis of sarcoidosis or treatment agents that may induce sarcoidosis. The patient was on infliximab and mycophenolate mofetil, both of which have many known cutaneous adverse effects. Given the high side effect profile of available treatment and limited data to support clinical efficacy, further study should be geared towards determining which of the immunosuppressive agents are best suited for treatment with the mildest adverse effect profile.






