Impact of Variableorientation and Flow Rates on Radiofrequency Ablation Lesions Created by Externally Irrigated Catheters: An Ex-Vivo Study
Nishaki Mehta†, Katerina Morgaenko†, William Sauer§, William Stevenson, David Haines‡
†Division of Cardiovascular Medicine, University of Virginia Health System, Charlottesville, Virginia.§Brigham and Women’s Hospital, Boston, Massachusetts, Vanderbilt Health System, Nashville, Tennessee.‡Beaumont Hospital, Oakland University of Medicine, Michigan.
The impact of variability in irrigation rates and catheter orientation on radiofrequency ablation (RF) lesion creation has not been studied systematically for the uniformly irrigated 56-pore (56P) catheter. This study aimed to analyze the impact of irrigation flow rates (IFRs) and catheter orientation (CO) settings on RF lesions sizes produced by a 56P irrigation catheter in a power-controlled mode using an ex-vivo model. RF lesions were created in strips of chicken muscle in a saline bath heated to 37°C with 56P and 6P catheters using low flow rate (LFR) at 2 cc/min and standard flow (SFR) irrigation rates at 8 cc/min for 56P and 17 cc/min for 6P with horizontal (HO) and vertical (VO) catheter orientations. Ablation power of 20W was delivered for 30 seconds with a mean contact force of 10 g. Sixty RF lesions were analyzed. For the 56P catheter, in contrast to the 6P catheter lesion geometry was independent of CO and IFR in our model. Although 6P catheter had slightly deeper lesions, the overall lesion volumes were similar for 6P and 56P catheters. CO and IFR appeared to have minimal impact on lesion volume creation with 56P catheter. In head-to-head comparison the 6P and 56P irrigated catheters performed similarly.
Key Words : Ablation Biophysics, Low Flow Lesions, Catheter Orientation.
Dr. Nishaki Mehta, Division of Cardiovascular Medicine, University of Virginia Health System, Charlottesville, Virginia, 1215 Lee Street, Hospital Expansion, 4th floor, office 4000, Charlottesville, VA, 22908.
Radiofrequency ablation (RF) utilizes the delivery of high frequency alternating electrical current to myocardial tissue to create a thermal lesion1 RF lesion geometry is the result of a complex interaction between the ablation catheter configuration, energy delivery settings and tissue characteristics The 6 pore (6P) ThermoCool SmartTouch® and the 56 pore (56P) ThermoCool SmartTouch Surround Flow® are widely available externally cooled catheters with force sensing technology. The 6P irrigation system was approved for ablation in 2009 and has 6 circumferentially placed irrigation holes (0.40 mm diameter) at the distal end of the 3.5 mm ablation tipThe 56P catheter was developed and introduced in May 2015 to reduce irrigation flow rates and provide uniform cooling over larger surface area. This ablation catheter has 56 small (0.08 mm diameter) irrigated holes distributed uniformly around the distal electrode surface, intended to achieve a more uniform distribution of the irrigating solution and more homogenous electrode cooling We focused on recreating clinical parameters for AF ablation to test these two catheter platforms. The purpose of this study was to determine the relationship of the ablation parameters to lesion size and geometry comparing the two modes of electrode irrigation. To test these relationships, a superfused ex vivo tissue ablation model was selected.
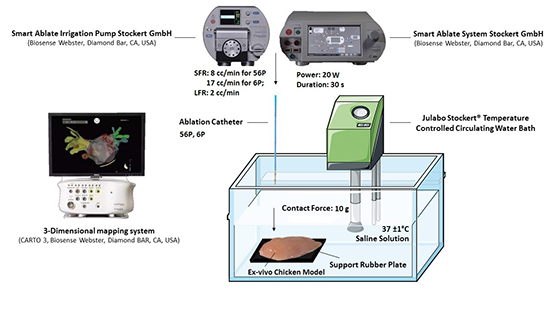
In this study the impact of catheter orientation (CO) and varying irrigation flow rates (IFRs) on the lesion sizes: depth, surface area and volume were examined. An ex-vivo chicken muscle model was immersed into the bath and allowed to equilibrate to 37 ± 1°C in a temperature-controlled circulating solution (Cobe, Julabo Stockert®, Germany). RF energy was applied in unipolar mode between catheter electrode and indifferent dispersive electrode placed at the bottom of the bath. Saline concentration of the superfusate was titrated to achieve a system impedance between 100 - 150 Ω. Commercially available ablation catheters with 3.5 mm tips and 56P (ThermoCool SmartTouch SF®, Biosense Webster Diamond Bar, CA, USA) and 3.5 mm tips and 6P (ThermoCool SmartTouch ®, Biosense Webster Diamond Bar, CA, USA) ablation catheters were used to deliver ablation energy (Stockert SmartAblate™ HF generator, Biosense Webster Diamond Bar, CA, USA). Saline irrigation was infused through the catheter with an external pump (SmartAblate™ System Pump, Biosense Webster Diamond Bar, CA, USA). During RF energy delivery, irrigation of the electrode was maintained at either low flow rate (LFR) 2 cc/min or at standard flow rate (SFR) 8 cc/min for the 56P catheter; and standard flow rate 17 cc/min for the 6P catheter. Ablation lesions were created in a power-control mode at 20 W delivered for 30 s with contact force (CF) at 10 g. These parameters were selected as they closely recapitulate clinical operating settings for atrial fibrillation ablation procedures CF was controlled via 3D mapping system (CARTO®, Biosense Webster Inc., Diamond Bar, CA, USA) [Figure 1]. A zero-force point for the CF sensor was calibrated prior to each application. Experimental conditions for all permutations of CO (horizontal and vertical) and IFR (low and standard) were iterated using 6P and 56P irrigated catheters. RF lesion measurements were obtained by the tissue dissection through the midpoint of the lesion. Lesion geometry was described with measured parameters: lesion depth, length and width, and calculated parameters: lesion volume and surface area. Lesion dimensions were measured using a digital caliper (0.01 mm resolution) and used to calculate the lesion volume and electrode surface areas. While there are several ways of determining lesion volumes, we followed the methodology from prior literature where chicken model was utilized and similar configurations were tested. 6,7
Figure 1. Illustration shows equipment and materials used for experimental setup.
Lesion volumes were calculated as half the volume of an oblate spheroid using the Eq.1, lesion surface area was calculated using ellipse equation Eq.2.
.
| lesion volume = (1) |
surface area = (2) |
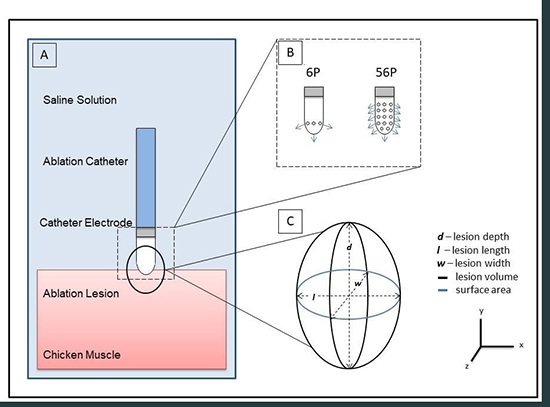
Where d is maximum lesion depth, l is lesion length, and w – width [Figure 2]. When a steam-pop occurred, RF was terminated and repeated at a different site under the same experimental settings. No lesions with steam pops were included in the systematic lesion dimension analysis because the steam pop disrupted the lesion geometry.
Figure 2. A: Schematic illustration of experimental model. B: Pore distribution of 6P and 56P irrigated catheters. C: Lesion geometry. Measured parameters: lesion depth, length and width. Calculated parameters: lesion volume and surface area.
A total of sixty RF lesions were created. The impact of varying catheter orientations (HO and VO) and IFR (SFR and LFR) for the 56P catheter operated in a power-controlled mode where ablation energy of 20 W was delivered for 30 s with mean CF of 10 g was analyzed. For the 56P catheter, recommended SFR was 8 cc/min, LFR was manually set to 2 cc/min. The total number of thirty lesions was analyzed in 56P. To perform a head-to-head comparison of the irrigated catheter designs under SFRs and differential CO, thirty lesions were created using the 6P catheter. Power of 20 W was delivered in power-control mode for 30 s with mean CF at 10 g under SFR for 6P at 17 cc/min.
Continuous variables were described as mean ± SD. Student t-test was used to compare lesion depths, surface areas and volumes. The effects of CO and IFR on lesion size were assessed by performing analysis of variance ANOVA for differences within groups. A p-value < 0.05 was considered significant.
. Catheter orientation had minimal effect on lesion characteristics for the 56P catheter.
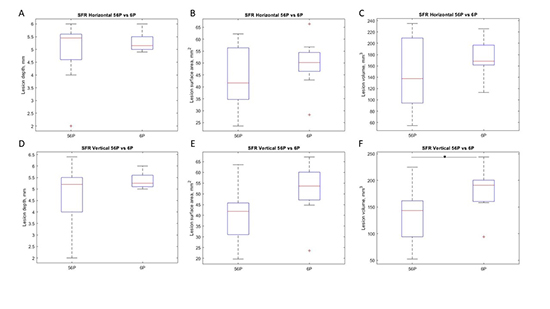
There was no significant difference in lesions with varying catheter orientations on lesion depth, surface area or volume for SFR and LFR in the vertical (VO) and horizontal orientations (HO) . The lesion depths for SFR VO, SFR HO, LFR VO and LFR HO were 4.7± 1.6, 4.9 ±1.1, 4.6± 1.1 and 4.4 ±1.2 mm respectively. (p>0.05) The lesion surface area for SFR VO, SFR HO, LFR VO and LFR HO were 44.8 ±12.2 44.3± 16.3, 57.1 ±11.2 and 55.8 ±15.8 mm2 respectively.(p>0.05) The lesion volumes for SFR VO SFR HO, LFR VO and LFR HO were 143.6± 56.6, 151.8± 75.1 , 176.8 ±57.8 and 168.2 ± 76 mm3 respectively. (p>0.05) [Figure 3].
Figure 3. This panel shows the impact of catheter orientation and irrigation flow rates for 56 P catheter for lesion depth, surface area and volume. A: Lesion depth were similar between varying COs and IFRs, all p > 0.05. B: In VO lesion surface area was significantly larger in LFR (2cc/min) when compared to SFR (8 cc/min). Asterix indicates p < 0.05. C: Lesion volumes were similar among tested modalities, all p > 0.05.

. The impact of changing irrigation flow rates was minimal on lesion size.
While there was a slight increase in the surface area with LFR settings in VO, the overall lesion sizes were similar [Figure 3]. ANOVA test showed no difference in the depth and volume for given power despite change in catheter orientation and flow rates.
. Comparison of 6P catheter to 56P catheter showed similar lesion sizes.
Comparison of 6P catheter to 56P catheter showed similar lesion sizes. Overall, these catheters performed similarly, the 6P catheter tended to create deeper lesions. The lesion depths for 56P HO versus 6P HO was 4.9 ±1.1, and 5.3± 0.6 mm respectively. (p>0.05) The lesion depths for 56P VO vs. 6P VO was 4.7± 1.6 and 5.5 ±0.6mm respectively. (p>0.05) The lesion surface area for 56P HO versus 6P HO was 44.3± 16.3 and 52.3± 10.9 mm2 respectively.(p>0.05) The lesion surface area for 56P VO vs. 6P VO was 44.8 ±12.2 and 49.9± 12.5 mm2 respectively.(p>0.05).The lesion volumes for 56P HO versus 6P HO was 151.8± 75.1 and 172.1± 41.9 mm3 respectively.(p>0.05) The lesion volumes for 56P VO vs. 6P VO was respectively 143.6± 56.6 and 181.2 ±44.4 mm3. (p>0.05) [Figure 4].
Figure 4. Lesion created under SFRs (17 cc/min for 6P, 8 cc/min for 56P) with the catheters in HO and VO were compared between 6P and 56P catheter. A, D: Lesion depths were similar between 56P and 6P catheter in HO and VO, all p > 0.05. B, E: Lesion surface areas were similar among tested conditions, all p > 0.05. C: Lesion volumes were similar between 56P and 6P in HO, p > 0.05. F: In VO lesion volume was significantly larger for 6P, asterix indicates p < 0.05.
The present study analyzes the impact of different settings on lesion geometry for a 56P catheter. Our main findings are as follows:
. CO appears to have minimal impact on lesion sizes with 56P catheter.
. Similarly, IFR appeared to have no significant difference with 56P catheter
. In head-to-head comparison under similar power and CF settings, 6P and 56P created similar lesions with a trend for increased depth with 6P catheter.
Our goal was to systematically study a new catheter platform (56P), which is widely used with the conventional and studied catheter settings from a prior platform (6P). In AF ablation, the holy grail is to create a durable lesion mitigating risk of collateral injury, notably atrioesophageal fistulas. On strategy is to reduce power settings in the posterior wall where there has been a significant emphasis on posterior wall isolation as an AF trigger. 8,9,10 Hence, we selected a lower power setting to determine lesion characteristics with 6P and 56P using different configurations.
We studied the impact of CO on 56P and reviewed prior reports on the impact of CO on lesion geometry. 11,12,13 Wood et a elegantly demonstrated that lesion volumes were 26% and 31% smaller for the closed and open irrigated non-contact sensing platforms, respectively in HO compared to VO. Additionally, HO translated to lesser degree of electrode pressure per unit of surface. The impact on lesion surface area was not described. Interestingly, the impedance change was similar, as was also reported by Nagakawa et al In contrast to findings for the 6P catheter, lesion depth, surface area and volume appeared to be independent of CO in the 56P catheter. This is unlike the 6P irrigated platform where lesion sizes were larger, and non-irrigated platform where lesion sizes were smaller with the HO We postulate that these findings may be explained by a larger irrigation pore distribution in the 56P catheter, which could reduce the impact of CO as there could be significant reduction in the variability of the irrigation efficiency when the catheter is in HO. This could make the 56P platform function as a partially non irrigated platform when in contact with tissue in the horizontal orientation and might explain our observations. This could be advantageous in certain cardiac regions where manual dexterity in accomplishing desired catheter orientation may be limited.
Irrigation flow cools the electrode tip lowering the temperature at the electrode-tissue interface, thus reducing lesion sizePrevious reports suggest that higher IFR reduces lesion surface diameter compared to lower IFR but can permit higher power delivery into the tissue A prior study of Weiss et al. demonstrated that under similar experimental conditions to our study, higher IFR created smaller lesion surface diameters in 9-pore irrigated catheter operated in power-control mode with power delivery of 30 W per 30 s with CF of 10 g. 16 Interestingly, our findings suggested that the 56P platform supported marginally larger lesion surface area and volumes with LFR but overall had no significant difference with irrigation flow rates. This could be driven by the lower flow rates at baseline which further attenuates this difference when LFR settings were utilized.
Finally, while comparing 6P and 56P catheters, we noted that lesion sizes were similar. Our results appeared to be similar to findings by Winterfield et al who compared the impact of 6P, 56P and the Flexability catheter in a canine cardiac model, where overlap in lesion sizes created by different irrigated catheters including 6P and 56P was reported.17 However this study did not study the impact of catheter orientation and varying irrigation rates like we did. Based on the lesion dimensions, we postulate that the higher lesion depth with the 6P platform is offset by the larger surface area with the 56P at higher power settings, similar to findings from a prior study
While the principles that govern thermal lesion creation are the same as in vivo, the lack of circulating blood, contracting myocardium and clinical factors are important differences. Only acute lesion sizes can be assessed, and lesions may change over time during healing. The absence of blood precludes assessing the impact of charring and thrombus formation. We adjusted impedance in our saline bath to be similar between experiments with an addition of “as needed” salt introduction given our in vitro model and impedance measurements were not obtained owing to this. In addition, the lesions were assessed for size based on gross measurements. Whether this reflects the entire zone of ablation injury is a matter of debate and beyond the scope of the current manuscript. We did not analyze or log the steam pops which may have yielded further information but the lower power settings should render this less relevant. Future studies should evaluate this systematically.
Overall, the 56 P catheter appears to be less impacted by CO and IFR. In comparison to its predecessor 6P, 56P appears to comparably perform for lesion volumes at given settings.






