‘Heart Rate Deficit’ from Dysautonomia in a Bariatric Surgery Patient - An Unusual Cause of Recurrent Syncope
Rakesh Gopinathannair*#, Iftekhar Ahmed#, Krishna Akella*#, Luis Couchonnal¥, Ghulam Murtaza*#, Dhanunjaya Lakkireddy*#, Brian Olshansky€
*Kansas City Heart Rhythm Institute, Overland Park, KS.#HCA Midwest Health, Kansas City, KS.¥St. Joseph’s Hospital, Kansas City, MO.€University of Iowa Hospitals and Clinics, Iowa City, IA.
Rakesh Gopinathannair, MD, MA, FAHA, FACC, FHRS
Cardiac EP Lab Director, Kansas City Heart Rhythm Institute and Research Foundation
Professor of Medicine, University of Missouri-Columbia
Associate Professor of Medicine (Adjunct), University of Louisville
5100 W 110th St, Ste 200
Overland Park, KS 66211
Since development of laparoscopic sleeve gastrectomy in 1999, bariatric surgery (BS) for morbid obesity has become increasingly common due its minimally invasive nature in conjunction with demonstrated mortality benefit.1 The greatest weight loss occurs 6-24 months postoperatively.2,3 Patients undergoing bariatric surgery are prone to develop symptomatic autonomic dysfunction with associated orthostatic intolerance potentially causing syncope. 4,56 We report a case of bradycardia-mediated syncope without associated hypotension in a patient who had prior BS.
A 61-year-old female with hyperlipidemia, fibromyalgia, morbid obesity status post gastric sleeve surgery 2 years prior, was seen for recurrent episodes of syncope over the past 2 months. Patient had significant weight loss (~170 lbs.) post-surgery over the 2-year period. She began noticing increasing fatigue and exercise intolerance in the four months before syncope initiation. Episodes occurred while sitting and while standing but most occurred without prodrome.
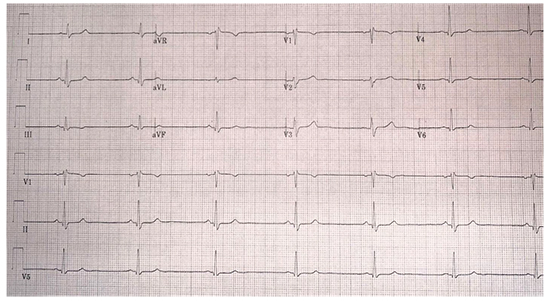
Baseline ECG showed sinus bradycardia at 41 bpm [Figure 1] with no other abnormalities. Thyroid function was normal. Other laboratory values were within normal limits. The echocardiogram was normal. During hospitalization, multiple syncopal episodes were witnessed while she tried to sit up or lift her head 30-60 degrees from a recumbent position. This was reproducible. Her baseline heart rate (HR) with telemetry monitoring was 36-42 bpm and her blood pressures were in the normal range (e.g., 126/78 mm Hg).
Figure 1. Baseline ECG at presentation showing sinus bradycardia at 41 bpm with normal QTc
During witnessed syncopal episodes, the HR remained unchanged (35-40 bpm) with no asystolic pauses. He eyes were closed. The systolic blood pressure also remained unchanged (120-140 mm Hg). Symptoms were so severe and was only relieved by either lying flat on the bed without a pillow or placing bed in a Trendelenburg position.
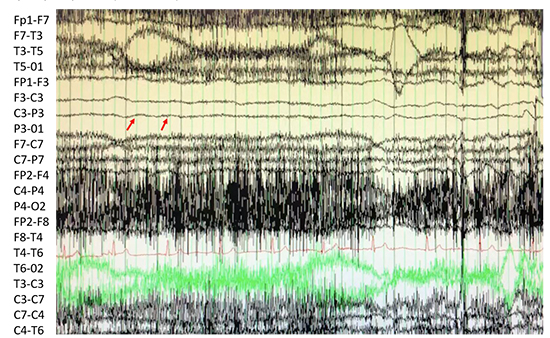
Psychogenic psuedosyncope was suspected given the unusual presentation. There was no history of psychological problems noted otherwise. However, video electroencephalogram showed loss of brain electrical activity during the syncopal episode [Figure 2]. No seizure activity was noted. No other cause for syncope was noted despite extensive investigation.
Figure 2. Video electroencephalogram showing loss of electrocerebral activity during the syncopal episode (red arrows)
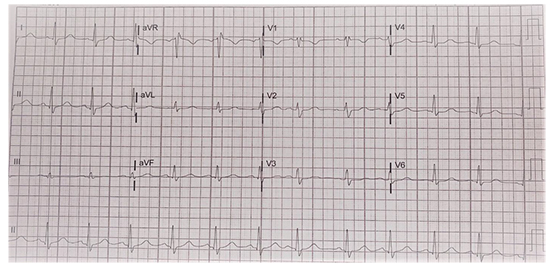
Review of prior ECGs during the peri-procedural period following bariatric surgery in 2017 showed a baseline HR ranging between 75-90 bpm [Figure 3]. Progressive decline in baseline HR since BS as well as baseline bradycardia raised concern for weight loss related dysautonomia and was suspected as a potential cause for syncope.
Figure 3. ECG obtained during peri-procedural period following bariatric surgery 2 years ago showing sinus rhythm at 72 bpm
She underwent a dual chamber permanent pacemaker implantation programmed MVP-R (AAIR>>DDDR) at 60-130 bpm along with rate drop response. Dramatic improvement was noted in her symptoms. She was discharged the following day as she was able to stand up and walk with no dizziness or orthostatic intolerance. Over a 7-month follow-up, she has not had any further recurrence of syncope and remains atrially paced.
Bariatric surgery has been increasingly used for patients with morbid obesity, and has been associated with improved outcomes. 1 Studies have shown changes in autonomic indices following BS, specifically an increase in vagal tone and relative vagal efferent flow after gastric bypass surgery.4,5 Studies on heart rate variability parameters following BS show that autonomic indices overall tend to change toward a parasympathetic predominance. 5,6 Multiple studies have reported on orthostatic intolerance 6 and associated symptoms following BS but little information is available regarding other mechanisms causing syncope. Moreover, exact mechanisms underlying autonomic dysfunction in these patients remain unclear. Whether the increased vagal tone is secondary to weight loss or another mechanism remains to be elucidated.6 Nerve redistribution during gastric bypass surgery as well as the impact of BS on various gut hormones such as insulin, leptin, ghrelin, gastrin, GLP-1, CCK has been proposed as potential mechanisms increasing vagal tone. 7 Multiple mechanisms thus may be in play which can alter the intricate autonomic balance following BS and create dysfunction.
We report, for the first time to our knowledge, a post-bariatric surgery patient where progressive weight loss resulted in progressive decline in baseline HR leading to recurrent, debilitating syncope without any long pauses/asystole or vasodepression. It appears that there was a relative ‘HR deficit’ where baseline HR fell below a critical threshold for adequate cerebral perfusion with any postural changes despite a blood pressure that remained within the normal range, both during recumbent position as well as with postural changes. Pacemaker implantation completely resolved symptoms by increasing base HR and restoring adequate cerebral perfusion. Further studies are needed to better understand mechanistic underpinnings behind progressive bradycardia without vasodepression following BS.
We describe a unique case where marked decline in resting HR occurred in association with significant weight loss following bariatric surgery. This ‘HR deficit’ and resting bradycardia, likely due to dysautonomia, resulted in recurrent syncope without asystole or vasodepression, and completely resolved with permanent pacemaker implantation.






