Demographic Characteristics and Patterns of Medication in Atrial Fibrillation Patients in South West Ontario: Insights from a Large Primary Care Database
Robert J Petrella, MD, PhDa, Luc Sauriol, PhDb
aDepartment of Family Medicine and Cardiology, The University of Western Ontario Lawson Health Research Institute, 801 Commissioners Rd East, Suite B-3002, London, Ontario, N6C 5J1, Canada
.bManager, Health Economic and Health Outcomes, Sanofi Aventis Canada,2150 St-Elzéar Ouest, Laval, Qc, H7L 4A8
.
Information about current practice in primary care-based management of atrial fibrillation (AF) can help to improve care quality.
To assess the epidemiology of AF and current patterns of treatment in order to identify therapeutic trends and aspects of current practice that may allow for care-gap identification.
We scrutinized the anonymized records of the South Western Ontario database (SWO) collected between July 2002 and October 2008 for information about the characteristics and management of AF patients.
From a population of ~168,000 patients we identified 4922 patients with a diagnosis of AF (2.9%). The recorded prevalence of AF increased with age, from <2% at age <60 years to 6% in the age range 71–75 years and 10% at age ≥81 years. AF patients were characterized by an unfavourable cardiovascular risk profile including widespread hypertension (54% of all cases), coronary artery disease (37%) and heart failure (21%), many cases of which were advanced (New York Heart Association class III or IV). Diabetes (22%) and dyslipidaemia (31%) were also widely prevalent.
The most frequently prescribed anti-arrhythmic drugs (AADs) were sotolol (n=798), amiodarone (n=712) and propafenone (n=451). Recorded use of flecainide was relatively low (n=175). Rate control-agents were being prescribed for 1838 patients, beta-blockers for 1311 patients and calcium channel blockers (CCBs) for 784 patients.
Use of anticoagulants was higher among patients assigned to AADs than among those assigned to rate-control drugs (>25% vs. ~10%). Overall prescription rates for other concomitant medications were >50% for ACE inhibitors/ARBs, 30–35% for statins and beta-blockers, and 27–29% for diuretics, digoxin and CCBs.
These Canadian patients with AF were relatively elderly and had multiple concomitant cardiovascular conditions and medications.
Correspondence to: Robert J Petrella MD, PhD, FCFP, FACSM, Beryl and Richard Ivey Research Chair, Lawson Health Research Institute, Assistant Director, Family Medicine and Cardiology, The University of Western Ontario,801 Commissioners Rd East, Suite 3002, London, Ontario, N6C 5J1, Canada
Management of patients with AF represents a substantial challenge by virtue of the complexities of the condition, the need for multiple therapies to address all aspects of AF-related risk and the number of patients who are candidates for treatment. Although rhythm control has traditionally been regarded as the definitive clinical response, several large controlled trials comparing these approaches have shown no significant differences in major endpoints including mortality and current expert guidelines recognize a role for both approaches.3-5
Coincidentally, it is recognized that the prevention of hospitalization due to cardiovascular causes and the avoidance of treatment-related toxicities may be at least as relevant to AF management as the prevention of recurrence of AF.
These considerations form part of the background to the present study, which had the objective of assessing the epidemiology of AF and current patterns of treatment in order to identify therapeutic trends and aspects of current practice that may allow for care-gap identification. Accordingly, we examined the South Western Ontario (SWO) primary care database to gain insights into the demographics of AF patients in this cohort and patterns of drug therapy for AF.
The SWO database contains anonymized health-related information about >225,000 adult patients in rural and urban primary care practices in south-western Ontario, with a total population of about 1.5 million people. The SWO thus contains data on ~20% of the region’s inhabitants.
The SWO was established in 2000; there are currently 53 participating primary care practices and >225,000 patients records are maintained. Previous studies have described the generalizability of the cohort to Canadian health data. 6 Baseline records were established for all participating patients documenting demographic, complete morbidity profile, medications, and other clinical data. Thereafter, the cohort database has been updated quarterly in response to clinical activity/events, including hospitalizations, morbidity and mortality. The trigger for an update is a billed patient encounter. Data collated into the SWO are extracted from charts at point of care, and then entered into a proprietary Structured Query Language (SQL)TM program which includes data verification. Data collection is conducted by a designated data abstraction team who also conducts verification on a random sample of 10% of records quarterly. Error rates are less than 1.3% per annum. Phase 1 of this interrogation of the SWO database was conducted using data collected between 1 July 2002 and 18 October 2008. Objectives for this first 1 July 2002 and 18 October 2008. Objectives for this first phase included the development of demographic profiles for AF patients prescribed rhythm- or rate-control drugs. Specific items of epidemiology included age, gender, weight, type of AF, creatinine level, cardiovascular history, co-morbidity and concomitant medications. Presence of AF was identified by at least one of the following: using ICD-9/10 coding for AF; text entry for AF (atrial fibrillation, arrhythmia-atrial, rhythm disturbance-atrial or supraventricular) and cross-referenced with medication prescribed for AF.
In the second part of our investigation we extracted epidemiological and demographic data for all patients who had a diagnosis of AF and sought to relate patterns of AF drug therapy with major clinical events such as emergency presentation, hospitalization and toxicity incidents presumed due to use of anti-arrhythmic agents.
During the period of our review the SWO accrued information on 168,023 patients. Our inspection identified 4922 patients with a diagnosis of AF (2.9% of the total population). The age distribution of those patients differed markedly from the non-AF contingent of the SWO (n=163,101).Thus, only six patients younger than 36 years of age had a diagnosis of AF and fewer than 3% of all AF cases (n=141) were identified in patients under the age of 46 years. Conversely,69.4% of AF patients were ≥71years old, compared with 23.8% of the non-AF cohort, and 40.6% of the AF patients were ≥81 years old (cf. 11.4% in the non-AF cohort).The recorded prevalence of AF increased with age, from less than 2% at age <60 years to 6% in the age range 71–75 years and 10% at age ≥81 years (Figure 1).Summary demographic particulars of the AF cohort, including the age distribution and classification of AF (persistent, permanent or paroxysmal) are presented in Table 1.
Figure 1. (a): Age distribution of patients in the SWO with a diagnosis of AF (n=4922); (b) Prevalence of AF by age
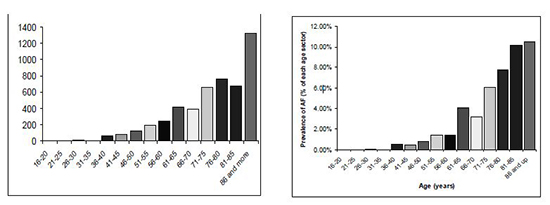
Table 1. Demographic and clinical details of the 4922 patients with a case record of AF
| Mean age (years) |
74 |
| Males (%) |
50% |
| Mean weight (kg) |
74kg |
| Average creatinine level (uM/L) |
137 |
| CV history |
| Hypertension |
2637 |
| CHF |
1025 |
| NYHA Class 1 |
121 |
| NYHA Class 2 |
180 |
| NYHA Class 3 |
337 |
| NYHA Class 4 |
387 |
| Coronary heart disease |
1821 |
| Diabetes |
1079 |
| Dyslipidaemia |
1542 |
| Concomitant medications |
|
| Oral anticoagulant |
2235 |
| Beta-blockers |
1717 |
| ACEI / ARBS |
2751 |
| Diuretics |
1432 |
| Digoxin |
1358 |
| Calcium channel blockers |
1337 |
| Statins |
1478 |
| NSAID |
603 |
CV – Cardiovascular; CHF – Coronary Heart Failure; NYHA – New York Heart association; ACEI – Angiotensin-converting enzyme inhibitor; ARBS – Angiotensin receptor blockers; NSAID – Non-steroidal anti-inflammatory drugs
Patients Receiving Anti-arrhythmic Drugs
Eighty percent of patients in the AF cohort (n=3443) were recorded as receiving one or more anti-arrhythmic drugs (AADs).
Table 2 displays data for these 3443 patients, stratified according to the recorded use of AADs. Overall the cohort was elderly (mean age 78 years) with a small preponderance of men. Hypertension was widely prevalent and just over a quarter of the patients had congestive heart failure (CHF), predominantly (n=685; ~70%) in New York Heart Association (NYHA) class III or IV. Diabetes, dyslipidaemia and coronary artery disease were widely prevalent and there was extensive polypharmacy.
Table 2. Demographic and clinical data for patients with a case record of AF, stratified according to the recorded use of AADs. (Percentage may exceed 100 for NHYA classes 1–4 because status was often recorded as NYHA 2–3 or NYHA 3–4, with information then entered in both cells.)
|
Any AAD(N=3443) |
AMIODARONE(n=712) |
SOTALOL (n=798) |
PROPAFENONE(n=451) |
FLECAINIDE(N=176) |
OTHER(n=558) |
| Mean age (years) |
78 |
80 |
79 |
89 |
76 |
75 |
| Males (%) |
53% |
63% |
50% |
58% |
67% |
47% |
| 79kg |
91kg |
77kg |
75kg |
80kg |
77kg |
| Average creatinine level (uM/L) |
134 |
127 |
136 |
130 |
141 |
| Type of AF (persistent; paroxysmal; permanent) % |
44%; 38%; 18% |
41%; 21%; 38% |
44%; 35%; 21% |
39%; 31%; 30% |
43%; 42%; 15% |
35%; 49%; 16% |
| Males (%) |
50% |
Males (%) |
50% |
Males (%) |
50% |
50% |
| CV history |
|
|
|
|
|
|
| Hypertension |
2109 |
674 |
663 |
212 |
73 |
357 |
| CHF |
973 |
275 |
248 |
79 |
3 |
300 |
| NYHA Class 1 |
114 |
6 |
8 |
1 |
0 |
99 |
| NYHA Class 2 |
170 |
38 |
50 |
7 |
1 |
74 |
| NYHA Class 3 |
319 |
94 |
81 |
20 |
2 |
122 |
| NYHA Class 4 |
366 |
137 |
109 |
51 |
0 |
69 |
| 1394 |
397 |
581 |
112 |
73 |
291 |
| Diabetes |
886 |
188 |
315 |
12 |
23 |
370 |
| Dyslipidaemia |
1013 |
415 |
423 |
123 |
62 |
100 |
| Concomitant medications |
|
|
|
|
|
|
| Oral anticoagulant |
1233 |
330 |
521 |
113 |
82 |
267 |
| Beta-blockers |
348 |
184 |
12 |
101 |
77 |
50% |
| ACEI / ARBS |
1488 |
339 |
224 |
124 |
131 |
799a |
| Diureticsa |
775 |
236 |
220 |
26 |
82 |
293b |
| Digoxin |
937 |
121 |
486 |
22 |
14 |
308 |
| Calcium channel blockers |
847 |
301 |
167 |
36 |
27 |
263 |
| Statinsb |
1263 |
429 |
391 |
116 |
62 |
278c |
| NSAID |
539 |
218 |
167 |
51 |
91 |
103 |
AAD – Anti-arrythmic drugs; AF – Atrial Fibrillation; CV – Cardiovascular; CHF – Coronary Heart Failure; NYHA – New York Heart association; ACEI – Angiotensin-converting enzyme inhibitor; ARBS – Angiotensin receptor blockers; NSAID – Non-steroidal anti-inflammatory drugs; a = Large N due to intra-class use, and ACE/ARB concomitant use, and switching; b = All classes/combinations of diuretics included; c = Includes switching and combinations
There were deviations from this overall pattern within sub-sets of patients receiving specified AADs. Hypertension and dyslipidaemia were markedly more prevalent than average in patients with prescription records for amiodarone or sotalol, as was a history of coronary artery disease. High-grade (NYHA III or IV) heart failure was conspicuous among the amiodarone sub-set. Conversely, both CHF and other major risk factors for cardiovascular disease were noted only infrequently in patients recorded as receiving either propafenone or flecainide. Patients receiving propafenone were noticeably older on average (80 years) than patients in other specified sub-groups. The proportion of men receiving flecainine was 67%, higher than the average.
Patients recorded as receiving ‘Other’ AADs had a marked prevalence of diabetes and coronary artery disease.
Anticoagulant use was higher than average in the amiodarone and sotalol sub-sets (Table 2). Concomitant use of beta-blockers was higher than average in patients receiving amiodarone or propafenone (~26% vs. ~10%, respectively). In all sub-sets except the flecainide group there was extensive use of ACE inhibitors/ARBs in relation to the proportions of patients recorded as having CHF. Use of diuretics appeared to be relatively low in the propafenone group. Extensive use of digoxin (60% of patients) was recorded in the sotalol subgroup.
Within the subsets defined by recorded therapy in Table 2, patients receiving amiodarone or propafenone were more likely than others to have a diagnosis of permanent AF.
Patients Receiving Anti-arrhythmic Drugs
Among the 1838 patients recorded as receiving rate-control drugs, half had hypertension and one-third had CHF, though the severity distribution was less skewed towards higher NYHA classes than for some other sub-sets defined by drug use (Table 3). The prevalence of diabetes was lower (28%) in patients treated with beta-blockers than in those treated with rate-control agents (42%) or CCBs (53%), as was hypertension (38% vs. 50–55%) (Table 3). Use of concomitant statin or ACE inhibitor/ARB therapy was also lower among the beta-blocker cohort 6than in the rate-control or CCB sub-sets (Table 3).
Table 3. Demographic and clinical data for patients with a case record of AF, stratified according to the recorded use of rate-control drugs, beta blockers and calcium channel blockers
|
Rate control agents(n=1838) |
Beta blockers(n=1311) |
CCBs(n=784) |
| Mean age (years) |
76 |
71 |
69 |
| Males (%) |
58% |
48% |
49% |
| Mean weight (kg) |
83kg |
77kg |
67kg |
| Average creatinine level (uM/L) |
134 |
136 |
130 |
| Type of AF (persistent; paroxysmal; permanent) % |
37%; 46%; 17% |
43%; 45%; 12% |
31%; 49%; 20% |
| CV history |
|
|
|
|
|
|
| Hypertension |
924 |
495 |
429 |
| CHF |
640 |
118 |
522 |
| NYHA Class |
132 |
6 |
86 |
| NYHA Class 2 |
108 |
17 |
76 |
| NYHA Class 3 |
176 |
24 |
151 |
| NYHA Class 4 |
224 |
71 |
209 |
| Coronary heart disease |
1294 |
541 |
753 |
| Diabetes |
778 |
363 |
415 |
| Dyslipidaemia |
735 |
463 |
272 |
| Concomitant medications |
|
|
|
| Oral anticoagulant |
234 |
133 |
98 |
| Beta-blockers |
1136 |
1311 |
434 |
| ACE inhibitors / ARBS |
1384 |
707 |
1271 |
| Diureticsa |
457 |
471 |
1002 |
| Digoxin |
138 |
123 |
| Calcium channel blockers |
529 |
173 |
784 |
| Statinsb |
1843 |
646 |
723 |
| NSAID |
523 |
359 |
296 |
CCBs – Calcium channel blockers; AF – Atrial Fibrillation; CV – Cardiovascular; CHF – Coronary Heart Failure; NYHA – New York Heart association; ACE – Angiotensin-converting enzyme; ARBS – Angiotensin receptor blockers; NSAIDs – Non-steroidal anti-inflammatory drugs
Hypertension and diabetes were documented in >50% of patients receiving CCBs and almost all the patients in this sub-set (753 of 784) had a record of coronary heart disease. Two-thirds had CHF, a percentage considerably higher than in the AF cohort overall, and a high proportion of those patients (40%) had advanced (NYHA class IV) heart failure. Anticoagulants were prescribed for 13% of these patients. Digoxin use (16%) was higher than in patients receiving rate-control agents (8%) or beta-blockers (6%). Recorded use of ACE inhibitors/ARBs and of diuretics exceeded 100%, a finding that may reflect prescription of multiple drugs within these classes, or drug switching.
In all three categories of patients described in Table 3 the proportion of patients receiving anticoagulants was considerably lower than among patients prescribed at least one AAD (Table 2) (10–13% vs. 35%), whereas patients receiving flecainide were slightly less likely than the average to have a diagnosis of permanent AF. Paroxysmal AF was more apparent than average in the sub-sets of patients defined by use of rate control agents, beta-blockers or CCBs (Table 3). The recorded incidence of permanent AF was lower than average in patients treated with beta-blockers (12% vs. 18%).
The AF data from the SWO reported here provide insights into the current characteristics and real-life management of patients with AF in the most populous province of Ontario. They also offer opportunities to examine changes over time within Canada7,8 and to make some international comparisons. 9-13
We identified 4922 patients with a diagnosis of AF.As the SWO database is updated in response to billed patient encounters and as it was initiated 10 years ago some of our AF cases may be of long standing. Hence ours is not necessarily a profile of patients with new-onset AF. This may be one explanation for the finding that the average age of our patients was higher than reported by some other groups9,11,14. A delay in the time between first symptoms of AF and clinical diagnosis, as described by Aliot et al, 15 may also have contributed to this situation. Of note in this context is a recent analysis of the Régie de l’assurance maladie du Québec (RAMQ) database, which describes a demographic profile similar to our own in a random sample of >66,000 AF patients first diagnosed between January 1998 and April 2009.
Our AF cohort comprised 50% female patients. This is a higher proportion of women than is usually reported but is consistent with the findings of the RAMQ analysis and some other reports. The relative predominance of women at the upper end of the age distribution is a factor in this finding. This observation might also be an indication of greater attention to the management of AF in women, which we would see as a positive trend.16 The aggregate prevalence rate of AF in our population (2.6%) was in line with other reports based on Canadian research. 8,17 The prevalence of AF in our cohort increased very markedly with age, especially after age 70 years. This finding was fully in accordance with expectations and with other reports.8,18
Our AF population was characterized by high rates of cardiovascular morbidity and by the presence of other conditions associated with poor prognosis in AF. In particular, there was widespread hypertension (54%) and a substantial number of patients with heart failure, which in many cases was well advanced (Table 1). Hypertension was recorded in 54% of our patients. This is similar to the rate reported in the ATRIA study. The profile of concomitant diseases likely to impact overall cardiovascular risk was substantially worse in our patient population than in the Canadian Trial of Atrial Fibrillation (CTAF) .19 This may reflect a general deterioration in risk profile of the Canadian AF population during the years since the CTAF study was completed or selection bias arising from CTAF exclusion criteria. The latter seems to us a more likely explanation and one that highlights the information value of an all-comers registry. There is strong correspondence between the cardiovascular disease profile of our population and that of the RAMQ.
The diagnoses of AF as paroxysmal, persistent or permanent in the SWO database are fluid and may change (forwards or backwards) over time. This is fully consistent with the ‘3P’ conception of AF that prevailed when the database was started 20and which continues, with some modification, today,3 however, this concept can complicate the interpretation of medication patterns and underlying prescriber motives. Rate control appears to have been the central aim of therapy, regardless of whether the means to that end was ‘pure’ rate-control drugs or drugs with both rate- and rhythm-control applications. The extensive use of amiodarone and sotalol suggests that physicians appreciate the value of drugs that combine rhythm- and rate-control effects, perhaps especially in medically complex cases. The extensive use of sotalol might, for example, be indicative of an emphasis on rhythm control in patients with concomitant conditions such as hypertension and coronary artery disease (Table 2). Most (79%) of SWO patients being prescribed amiodarone were recorded as having persistent or permanent AF and 33% had heart failure in NYHA class III or IV. Prescription rates increased with age. Given that our data were accrued over several years it is possible that some of the amiodarone-treated patients had lapsed into permanent AF and were receiving amiodarone for rate control; this would represent inappropriate use of the drug when better-tolerated alternatives are available. Alternatively, these patients may have had concomitant conditions that individual physicians regarded as warranting continuance of amiodarone therapy. The proportion of patient’s co-administered beta-blockers was relatively low.20
Despite having an average age of 76 years, patients recorded as receiving flecainide had a conspicuously better cardiovascular risk profile than other sub-sets in our analysis. These patients also had a higher proportion of paroxysmal AF. This profile would seem to be compatible with use of flecainide as a ‘pill-in-the-pocket’ strategy in selected patients, but our findings provide no definitive proof that such an express rhythm-control policy was in action.
The demographic profiles of patients assigned to rate control with either beta-blockers or CCBs were broadly similar apart from a very much greater use of CCBs in patients with heart failure. We currently have no explanation for this striking disparity, which is all the more notable given current recommendations on the use of beta-blockers in heart failure. Overall, beta-blocker use as a percentage of the whole SWO AF cohort was lower than might have been expected on the basis of the results of the CARAF I & II surveys.7
Usage rates for anticoagulants seems quite low given the generally poor cardiovascular health profile of our patients; this may be further evidence for the underuse of anticoagulation therapy in AF.21,22 We have no data on anticoagulation adequacy. Thus, even if the recorded prescription rates are shown to be an accurate appraisal of need, we cannot be certain that all patients who were candidates for anticoagulation received optimal therapy. We have no data on antiplatelet medications, and therefore cannot exclude the possibility that low rates of anticoagulant use may reflect the (possibly inappropriate) use of antiplatelet drugs.21
The low rates of digoxin use recorded in most categories of the SWO database (Table 2 & 3) likely represent a continuance of the trend of declining usage identified in the CARAF I & II surveys.7 The only exception to this finding was in the cohort of sotalol-treated patients, in which digoxin use was recorded in 61% of cases. These 486 patients accounted for more than half of all digoxin prescriptions.
Our database has various limitations. First, the study population is very old and the vast majority have co-morbid conditions. Nevertheless, the results from this study are valuable because they provide insights into real world data on the demographic characteristics of patients with atrial fibrillation. Second, we have no specific information about symptom severity associated with AF, or the frequency of symptomatic episodes. Symptomatology has an important influence on clinicians’ decision to aim for rate or rhythm control and, if attempting rate control, whether to impose strict or lenient goals. Lack of this information limits our capacity to interpret physicians’ intentions from prescription data. Third, we have no data on race or stroke incidence in participating patients. Fourth, we have no data on the use of electrical cardioversion or ablation procedures. We are therefore unable to comment on the interplay between pharmacological and non-pharmacological approaches to AF management.
In conclusion, the SWO is a very large real-world database that provides information likely to be broadly representative of the demographics of AF patients in Ontario and of the treatment these patients receive. Insights from the SWO can be used to inform future developments in the management of AF. In our primary analysis we identified 4922 patients (2.9% of the database population) with a diagnosis of AF; prevalence increased with age, reaching 10% at age ≥81 years. Our AF patients were characterized by an unfavorable cardiovascular risk profile. The most frequently prescribed AADs were sotalol (n=798) and amiodarone (n=712). Rate control-agents were being prescribed for 1838 patients.






