Operative Technique and Atrial Tachyarrhythmias After Orthotopic Heart Transplantation
Srinivasan Sattiraju1*, Shashank Vats1*, Balaji Krishnan1, Sun K. Kim2, Erin Austin2, Ilknur Can3, Venkatakrishna Tholakanahalli1, David G. Benditt1, Lin Y. Chen1
1Cardiac Arrhythmia Center, Cardiovascular Division, Department of Medicine, University of Minnesota Medical School, Minneapolis, MN 55455, USA;.2Division of Biostatistics, School of Public Health, University of Minnesota, Minneapolis, MN 55455, USA;.3Konya Üniversitesi Meram Tıp Fakultesi Kardiyoloji Konya, Turkey.
There is conflicting evidence that operative technique affects the risk of atrial tachyarrhythmia after orthotopic heart transplantation (OHT). We sought to determine whether OHT by bicaval (BC) technique is associated with a lower risk of atrial tachyarrhythmia than biatrial (BA) technique. Consecutive patients who underwent OHT between 1997 and 2007 at the University of Minnesota were included in this retrospective cohort study with follow-up through December 31, 2011. We included 260 OHT recipients (BA, 155; BC, 105). Fifty-nine patients (22.7%) developed early atrial tachyarrhythmias. The multivariable odds ratio (95% confidence interval [CI]) of BC technique for early atrial tachyarrhythmias was 0.85 (0.46-1.57), P=0.59. After a median follow-up of 4.9 years, 40 (15.4%) patients developed late atrial tachyarrhythmias. The multivariable hazard ratio (HR) (95% CI) of BC technique for late atrial tachyarrhythmias was 0.99 (0.50-1.96), P=0.98. Graft rejection was found to be a multivariate predictor of late atrial tachyarrhythmias (HR, 2.89; 95% CI, 1.48-5.65; P=0.002). In contrast to prior reports, we did not find an association between operative technique and early or late atrial tachyarrhythmias after OHT. Graft rejection is a risk factor for late atrial tachyarrhythmias after OHT.
Correspondence to: Lin Y. Chen, MD, 420 Delaware St SE, MMC 508, Minneapolis, MN, 55455.
Atrial tachyarrhythmias occur in the transplanted heart after orthotopic heart transplantation (OHT) with a reported incidence of 18% to 65%.1–3 While multiple factors may contribute, the post-operative atrial tachyarrhythmia risk may be due in part to the type of operative technique, specifically bicaval (BC) versus biatrial (BA) approach to anastomosis of the donor to recipient heart. The BA operative technique, with its anastomoses of donor and recipient atria, results in substantial distortion of normal atrial anatomy and requires long anastomoses in potentially excitable atrial tissues.4,5 By contrast, the BC method tends to preserve right and left atrial configuration; although the left atrium of the donor is anastomosed to a left atrial cuff of the recipient heart, the donor and recipient vena cava are directly anastomosed. The result is less extensive atrial surgery.6
Previous studies have examined the frequency of atrial arrhythmias in the two OHT operative techniques. While 2 studies7,8 reported less post-operative atrial tachyarrhythmias with BC method compared to BA, 2 other studies9,10 did not observe a significant difference. Consequently, we aimed to reassess the influence of OHT operative technique (BC vs. BA) on occurrence of early atrial tachyarrhythmias (≤30 days of heart transplanta tion) and late (>30days of heart transplantation) in a large cohort of OHT patients who underwent their operation within the last decade.
Patients who underwent OHT between 1997 and 2007 at the University of Minnesota were included in this retrospective cohort study. The present study is based on data obtained at baseline (date of OHT) and during follow-up through December 31, 2011. The protocol was approved by the University of Minnesota Institutional Board Review. Patients who underwent OHT at <18 years of age were excluded.
All available medical records were reviewed for demographics, indication for transplant, pre-transplant co-morbidities, and the type of operative technique (BC vs. BA). Additionally, we collected data on ECG-documented atrial tachyarrhythmias, and on occurrence of rejection episodes.
Indications for OHT were divided into ischemic (50%) and non-ischemic cardiomyopathy, and the latter was further characterized as dilated (37%), restrictive (5%), hypertrophic (2%) and valvular pathologies (6%). Pre-transplant co-morbidities included hypertension, diabetes, hyperlipidemia, obstructive sleep apnea, coronary artery disease, peripheral vascular disease, and pre-transplantation atrial tachyarrhythmias, specifically atrial fibrillation (AF) and atrial flutter (AFL).
Early post-operative tachyarrhythmia was defined as occurrence of rhythm-documented AF, AFL, or atrial tachycardia (AT) lasting more than 30 seconds, within 30 days after OHT. Late post-operative tachyarrhythmia was defined as occurrence of rhythm-documented AF, AFL, or atrial tachycardia (AT) lasting more than 30 seconds, more than 30 days after OHT. Rhythm strips or 12-lead ECGs were obtained when a patient had symptoms of chest discomfort, shortness of breath, palpitations, dizziness, or physical signs of tachycardia or hemodynamic instability. The ECGs or rhythm
strips were assessed independently by 2 cardiologists. A diagnosis of AF was made when there was an irregularly irregular R-R interval with no discernible atrial activity. AFL was diagnosed when clear-cut ‘saw-tooth’ atrial activity at fixed rate of 240-320 beats/min was present in the inferior leads. AT required presence of a non-AFL atrial tachycardia with non-sinus P-wave axis.11
Data regarding the presence and grade of acute rejection episodes after OHT were collected from histopathology results on endomyocardial biopsy done as routine surveillance or as clinically indicated when acute rejection was suspected. International Society of Heart Lung Transplant (ISHLT) grading of acute cellular rejection was used to classify the grades described and antibody mediated rejection was termed as humoral.12 If an atrial tachyarrhythmia episode occurred within 2 weeks of an acute rejection, the former was classified as a rejection-related atrial arrhythmia.
Categorical variables are presented as number (%) and continuous variables are presented as mean +/- standard deviation. Student’s t-test and Fisher’s exact test were used to evaluate statistical significant difference in baseline clinical characteristics between BA and BC groups. To estimate the association of operative technique with risk of early post-operative atrial tachyarrhythmia, we calculated odds ratios (ORs) and 95% confidence intervals (CIs) using logistic regression models. For late post-operative atrial tachyarrhythmia, person-years at risk were calculated from the date of OHT until the date of late post-operative atrial tachyarrhythmia, death, or last follow-up, whichever occurred first. We used Cox proportional hazards models to calculate the hazard ratios (HRs) and 95% CIs of operative technique for late atrial post-operative tachyarrhythmia. We ran 2 models: Model 1 was adjusted for age and sex; and Model 2 was additionally adjusted for the following baseline covariates: pre-transplant atrial tachyarrhythmia, obstructive sleep apnea, coronary artery disease, hypertension, diabetes mellitus, peripheral vascular disease, and time-dependent graft rejection episodes. In the logistic regression models for early post-operative atrial tachyarrhythmia, we did not adjust for graft rejection because there were no graft rejection-related atrial arrhythmias within 30 days after OHT.
In addition, to identify other risk factors for early post-operative atrial tachyarrhythmia, we included age, sex, operative technique, pre-transplant atrial tachyarrhythmia, obstructive sleep apnea, coronary artery disease, hypertension, diabetes mellitus, and peripheral vascular disease in a multivariable logistic regression model. To identify predictors of late post-operative atrial tachyarrhythmia, we included all aforementioned variables plus graft rejection in a multivariable Cox proportional hazards model. The proportional hazards assumption was tested using time interaction terms and inspection of log negative log survival curves and was found not to be violated in all models.
Statistical analysis was performed using SAS version 9.2 (SAS Institute Inc., Cary, NC). All P values reported were 2-sided, and statistical significance was evaluated at the 5% level.
There were 260 OHT recipients included in the study. The mean age was 52.0 ± 11.8 years at time of transplant, and 58 (22.3%) were women. OHT was performed in 155 (59.6%) patients by BA anastomosis and in 105 (40.4%) patients by BC anastomosis. The mean hospital stay (time from OHT to discharge) was 20.6 ± 20.3 days in BA group and 20.5 ± 20.3 days in the BC group, and was not significantly different between the groups (P=0.87).
Baseline clinical characteristics of the patient population are shown in Table 1. There was no significant difference in distribution of pre-transplant co-morbidities between BA and BC groups. Table 2. shows the number of BA and BC procedures by year during 1997-2007. There were more BA than BC procedures performed each year except for 2005 and 2006.
Table 1. Baseline Characteristics of Study Patients
| Variable |
Biatrial Group (n=155) |
Bicaval Group (n=105) |
P valuea |
| Sex |
|
|
0.45 |
| Male |
123 (79.4) |
79 (75.2) |
|
| Female |
32 (20.7) |
26 (24..8) |
|
| Age at transplant (years) |
51.9 ± 11.4 |
51.8 ± 12.3 |
0.98 |
| Hypertension |
69 (44.5) |
53 (50.5) |
0.38 |
| Hyperlipidemia |
63 (40.6) |
51 (48.6) |
0.25 |
| Obstructive sleep apnea |
12 (7.7) |
16 (15.2) |
0.07 |
| Diabetes mellitus |
47 (30.5) |
28 (26.7) |
0.58 |
| Coronary artery disease |
62 (40.0) |
33 (31.4) |
0.19 |
| Pre-transplant AF/AFL |
29 (18.7) |
26 (24.8) |
0.28 |
| Peripheral vascular disease |
10 (6.5) |
7 (6.7) |
1.00 |
aStudent t test was used to compare continuous variables which are expressed as mean ± SD. Fisher exact test was used to compare categorical variables which are expressed as number (%). AF, atrial fibrillation; AFL, atrial flutter.
Table 2. Number of Biatrial and Bicaval Procedures by Year
| Year of Transplant |
Number of Biatrial procedures (n=155) |
Number of Bicaval procedures (n=105) |
Total |
| 1997 |
3 (50.0%)a |
3 (50.0%)a |
6 |
| 1998 |
10 (58.8%) |
7 (41.2%) |
17 |
| 1999 |
8 (66.7%) |
4 (33.3%) |
12 |
| 2000 |
10 (62.5%) |
6 (37.5%) |
16 |
| 2001 |
7 (50.0%) |
7 (50.0%) |
14 |
| 2002 |
31 (86.1%) |
5 (13.9%) |
36 |
| 2003 |
27 (93.1%) |
2 (6.9%) |
29 |
| 2004 |
19 (51.4%) |
18 (48.6%) |
37 |
| 2005 |
11 (34.4%) |
21 (65.6%) |
32 |
| 2006 |
8 (34.8%) |
15 (65.2%) |
23 |
| 2007 |
21 (55.3%) |
17 44.7%) |
38 |
aAll percentages are row percentages
Early post-operative atrial tachyarrhythmias
Of 260 patients who underwent OHT, 59 (22.7%) developed atrial tachyarrhythmias within 30 days after surgery. Of the 59 patients, 42 (16.2%), 11 (4.2%), and 15 (5.8%) developed AF, AFL, and AT,respectively. Seven patients were affected by 2 types of atrial tachyarrhythmias and 1 patient had all 3 types. The OR (95% CI) for early atrial tachyarrhythmias associated with BC technique was 0.85 (0.46-1.57), P=0.59 after adjusting for age, sex, and other risk factors (Table 3., Model 2). In a multivariable logistic regression model, there were no baseline variables that significantly increased the odds of earlypost-operative atrial tachyarrhythmias (Table 4.).
Table 3. Risk of Early Post-Orthotopic Heart Transplant Atrial Tachyarrhythmias by Operative Technique
|
|
Biatrial (n=155) |
Bicaval (n=105) |
P value |
| P value |
|
|
|
|
| Number of events |
|
37 |
22 |
|
| Odds ratio (95% CI) |
Model 1a |
1 [Referent] |
0.85 (0.47-1.54) |
0.58 |
|
Model 2b |
1 [Referent] |
0.85 (0.46-1.57) |
0.59 |
aAdjusted for age and sex, bModel 1 additionally adjusted for pre-transplant atrial tachyarrhythmia, obstructive sleep apnea, coronary artery disease, hypertension, diabetes mellitus, and peripheral vascular disease. CI, confidence interval
Table 4. Logistic Regression Model for Risk of Early Post-Orthotopic Heart Transplant Atrial Tachyarrhythmias
| Variable |
Odds ratio (95% CI) |
P value |
| Operative technique (bicaval vs. biatrial) |
0.85 (0.46-1.57) |
0.59 |
| Age at transplant (per year) |
1.00 (0.97-1.02) |
0.87 |
| Sex (male vs. female) |
0.99 (0.48-2.08) |
0.99 |
| Pre-transplant AF/AFL |
1.23 (0.59-2.57) |
0.58 |
| Obstructive sleep apnea |
0.43 (0.13-1.36) |
0.15 |
| Coronary artery disease |
0.87 (0.45-1.68) |
0.67 |
| Hypertension |
1.71(0.93-3.17) |
0.09 |
| Diabetes mellitus |
1.53 (0.78-3.01) |
0.22 |
| Peripheral vascular disease |
1.35 (0.43-4.29) |
0.61 |
AF, atrial fibrillation; AFL, atrial flutter; CI, confidence interval.
Late post-operative atrial tachyarrhythmias
During a median (interquartile range) follow-up duration of 4.9 (2.3-7.3) years, 40 (15.4%) patients developed late post-operative atrial tachyarrhythmias. Of the 40 patients, 21 (52.5%), 15 (37.5%), and 12 (30.0%) developed AF, AFL, and AT, respectively. Eight patients had 2 types of atrial tachyarrhythmias and none had all 3 types.
During a median (interquartile range) follow-up duration of 4.9 (2.3-7.3) years, 40 (15.4%) patients developed late post-operative atrial tachyarrhythmias. Of the 40 patients, 21 (52.5%), 15 (37.5%), and 12 (30.0%) developed AF, AFL, and AT, respectively. Eight patients had 2 types of atrial tachyarrhythmias and none had all 3 types.were 3.3 and 2.9 per 100 person-years, respectively (P=0.71) (Table 5.) The multivariable HR (95% CI) for late post-operative atrial tachyarrhythmias associated with BC technique was 0.99 (0.50-1.96),
P=0.98 after adjusting for age, sex, and other risk factors (Table 5, Model 2). In a multivariable Cox proportional hazards model, graft rejection significantly increased the risk of late post-operative atrial tachyarrhythmias (HR, 2.89; 95% CI, 1.48-5.65; P=0.002) (Table 6).
Table 5. Risk of Late Post-Orthotopic Heart Transplant Atrial Tachyarrhythmias by Operative Technique
|
|
Biatrial (n=155) |
Bicaval (n=105) |
P value |
| Late atrial tachyarrhythmias |
Number of events |
26 |
14 |
|
| Person-years |
|
780 |
477 |
|
| Incidence rate |
|
3.33 |
2.94 |
0.71 |
| Hazard ratio (95% CI) |
Model 1b |
1 [Reference] |
0.91 (0.47-1.75) |
0.78 |
|
Model 2c |
1 [Reference] |
0.99 (0.50-1.96) |
0.98 |
aPer 100 person-years, bAdjusted for age and sex, cModel 1 additionally adjusted for pre-transplant atrial tachyarrhythmia, obstructive sleep apnea, coronary artery disease, hypertension, diabetes mellitus, peripheral vascular disease, and time-dependent graft rejection episodes.CI, confidence interval
Table 6. Cox Proportional Hazards Model for Risk of Late Post-Orthotopic Heart Transplant Atrial Tachyarrhythmias
| Variable |
Hazard ratio (95% CI) |
P value |
|
|
| Operative Report (bicaval vs. biatrial) |
0.99 (0.50-1.96) |
0.98 |
| Age at transplant (per year) |
1.00 (0.98-1.04) |
0.69 |
| Sex (male vs. female) |
1.04 (0.45-2.39) |
0.93 |
| Pre-transplant AF/AFL |
0.78 (0.34-1.81) |
0.57 |
| Obstructive sleep apnea |
0.76 (0.22-2.59) |
0.66 |
| Coronary artery disease |
1.23 (0.59-2.57) |
0.58 |
| Hypertension |
1.07 (0.54-2.10) |
0.85 |
| Diabetes mellitus |
1.16 (0.58-2.34) |
0.674 |
| Peripheral vascular disease |
0.87 (0.25-3.03) |
0.83 |
| Graft rejection |
2.89 (1.48-5.65) |
0.002 |
AF, atrial fibrillation; AFL, atrial flutter; CI, confidence interval
Post-operative atrial tachyarrhythmias, particularly AF, contribute substantially to length of hospitalization, cost of care, and long-term mortality following cardiac surgery,13–15 including in patients who have undergone OHT.8,16 The overall incidence of post heart transplant atrial arrhythmia in our study was similar to recently published contemporary data by Dasari et al17 with similar findings of higher incidence of first 30 days atrial arrhythmias as compared to post 30 days. The principal findings of our study are as follows. First, operative technique in OHT (BC versus BA) was not significantly associated with early or latepost-operative atrial tachyarrhythmias. Second, in multivariable analysis, graft rejection was found to be an independent predictor of late post-operative atrial tachyarrhythmias.
BC versus BA operative technique
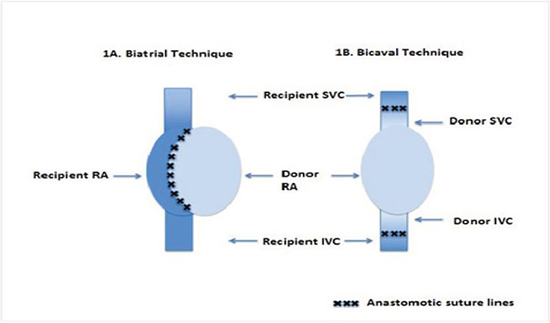
The BA technique was originally introduced by Lower and Shumway4,5 and remains the standard technique for OHT due to its simplicity. The BC method gained attractiveness in 1990’s with some studies suggesting that it decreased hospital stay, decreased pacemaker requirement, reduced atrial pressure, reduced tricuspid regurgitation, and had mortality benefit despite slightly longer ischemic times compared with the BA procedure.18,19 The BA technique (Figure 1A) involves the donor heart attached to right and left atrial cuffs of the recipient heart. In the BC technique (Figure 1B), the anastomoses are made at the level of vena cavae and a small recipient left atrial cuff around the pulmonary veins. The BA technique causes more distortion of the atrial anatomy and thereby a potential to produce a more arrhythmogenic substrate as compared to the BC technique.4,5
Figure 1. Figure 1A. Biatrial Technique, Figure 1B. Bicaval Technique, RA, Right Atrium; IVC, Inferior Vena Cava; SVC, Superior Vena Cava.
Data from prior studies have been inconsistent with regard to the risk of post-operative atrial tachyarrhythmias comparing BC and BA techniques. Certain prior prospective studies8,20–22 with relatively small sample sizes (30-75 patients in BA or BC) compared the burden of early atrial arrhythmias after OHT. These studies reported fewer atrial tachyarrhythmias with BC group as compared with BA. In contrast, Grande et al9prospectively studied 71 subjects in BA and 46 subjects in BC group after OHT and observed no significant difference in burden of AF between the groups (incidence of AF in BA 13.1% and BC 4.6%, P=NS). Khan et al24 reported incidence of AF in a large cohort of heart transplant patients and although the overall rate of post transplant AF was 0.3%, much lower compared to our study, the only cases of AF found were in the BC group. Cui et al 10 reported 13.1% incidence of AF in a larger population of 892 patients after OHT with 69 of 117 episodes of AF occurring within 2 weeks of transplantation. This study provided further evidence that BC group did not have any advantage over BA with respect to atrial tachyarrhythmia burden.
Considering the inconclusive literature regarding the relationship of post-operative arrhythmias to BC versus BA methodology, we sought to reassess this issue in an 11-year retrospective cohort of 260 OHT recipients at the University of Minnesota. During this 11-year period, there were more BA than BC procedures performed each year except for 2005 and 2006. In our study, we did not find a statistically significant difference between the 2 groups with respect to early post-operative arrhythmias. Although, there is no difference in early post-operative arrhythmias between the 2 operative techniques, there may be a difference in long-term arrhythmia outcomes. Indeed, a meta-analysis of several prospective and retrospective studies with longer follow-up periods19 suggested superiority of BC technique over BA technique in maintaining sinus rhythm. Thus, over time, BA operative technique may induce formation of the substrate necessary for generation of late post-operative atrial arrhythmias, particularly AF. However, in our study, we did not find a statistically significant difference between the 2 groups with respect to late post-operative arrhythmias.
Predictors of Post-Operative Atrial Trachyarrhythmias
Pre-transplant AF or AFL was not associated with an increased risk of post-operative atrial tachyarrhythmias probably because the prior cardiac substrate is removed during OHT. On the other hand, although hypertension and diabetes remain as potential risk factors, they did not influence the risk of early or late atrial arrhythmias. Consistent with the findings of previous studies,10,16,23,25 we found that graft rejection was significantly associated with an increased risk of late post-operative atrial tachyarrhythmias. One could postulate that graft rejections lead to fibrosis or edema, which in turn, set up heterogeneities in conduction or repolarization within the atria, promoting atrial tachyarrhythmias.
There are several limitations in our study. First, it is possible that asymptomatic arrhythmias might have been missed or were not documented. Second, factors that impact on the frequency of atrial tachyarrhythmias such as volume status, renal function, peri-operative infections, and immunosuppressive medical regimens were not included in the study. Additionally, factors that can increase the incidence of atrial arrhythmias in the first 30 days after surgery such as peri-procedural medications, hemodynamic changes, and metabolic derangements were not studied. Third, since this was a retrospective study, standardization of medical management that could impact on post-operative arrhythmic burden differences between BC and BA groups prior to or after OHT was not possible. Data on angiotensin receptor inhibitors or beta blockers use that could have anti-arrhythmic effects were not included in our study; our patients often had dynamic medical regimens prior to OHT, with these medications being held on several occasions for a significant period and with concomitant use of pressors and/or inotropes, making it impractical to include them for comparison between BC and BA groups. Fourth, data regarding the timing of atrial arrhythmias in relation to onset of graft rejection was not included in the study. Fifth, factors such as duration of transplant surgery, ischemia time of the donor heart, and co-morbidities of the donor that can potentially impact development of post-transplant atrial arrhythmias were not studied. Finally, we did not characterize the type of AF in our patients, i.e., paroxysmal, persistent, or permanent AF nor did we assess frequency burden of atrial arrhythmias.
Our study indicates that susceptibility to early or late post-OHT atrial tachyarrhythmias is not significantly different whether BC or BA operative technique is employed for OHT. Graft rejection is significantly associated with late post-transplant atrial tachyarrhythmias.
No disclosures relevant to this article were made by the authors.






