Performance of the Cockcroft-Gault, MDRD and CKD-EPI Formulae in Non-Valvular Atrial Fibrillation: Which one Should be Used for Risk Stratification?
Sérgio Barra1, Rui Providência2,3,4, Catarina Faustino3, Luís Paiva3, Andreia Fernandes3, António Leitão Marques3
1Cardiology Department, Papworth Hospital NHS Foundation Trust, Papworth Everard,Cambridge CB23 3RE, UK.2Cardiology Department, Clinique Pasteur,Toulouse,France.3Cardiology Department, Coimbra’s Hospital and University Centre, Coimbra,Portugal.4Cardiology Department, Faculty of Medicine, University of Coimbra,Coimbra,Portugal.
Renal dysfunction is a strong predictor of adverse events in patients with atrial fibrillation (AF). The Cokcroft-Gault, Modification of Diet in Renal Disease (MDRD) and Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) equations are available for estimating the glomerular filtration rate (GFR). No comparisons between these equations have yet been performed in patients with non-valvular AF concerning their mid-term prognostic performance.
Cross-sectional study of 555 consecutive patients with non-valvular AF undergoing transesophageal echocardiogram. We tested the prognostic performance of the aforementioned GFR estimation formulae, namely their ability to predict all-cause mortality (primary endpoint) and major cardiac adverse or ischemic cerebrovascular events (secondary endpoints) during an average follow-up of 24 months.
Regarding the primary endpoint, Cockcroft-Gault (AUC=0.749±0.028) was superior to both MDRD (AUC=0.624±0.039) and CKD-EPI (AUC=0.641±0.034) [p<0.001 both comparisons] while CKD-EPI was superior to MDRD (p=0.011). Cockcroft-Gault was marginally superior to both MDRD (AUC=0.673±0.049 vs. AUC=0.586±0.054, p=0.041) and CKD-EPI (AUC=0.673±0.049 vs. AUC=0.604±0.054, p=0.063) in the prediction of ischemic cerebrovascular events, while no difference was found between CKD-EPI and MDRD. Concerning AUC for prediction of MACE, Cockcroft-Gault was superior to MDRD (p=0.009) and CKD-EPI (p=0.012), while CKD-EPI was similar to MDRD (p=0.215). Multivariate predictive models consistently included Cockcroft-Gault formula along with CHADS2, excluding the other two equations. Measures of reclassification revealed a significant improvement in risk stratification for all studied endpoints with Cockcroft-Gault instead of CKD-EPI.
In patients with non-valvular AF, the Cockcroft-Gault more appropriately classified individuals with respect to risk of all-cause mortality, ischaemic cerebrovascular event and major adverse cardiac event.
Key Words : Atrial fibrillation, renal dysfunction, risk prediction, stroke, mortality.
Corresponding Address :
Sérgio Nuno Craveiro Barra, Cardiology Department, Papworth Hospital NHS Foundation Trust, Papworth Everard, Cambridge CB23 3RE, UK
Atrial fibrillation (AF) is the most common sustained arrhythmia and associates with increased risk of stroke and all-cause mortality. Currently used risk stratification schemes such as CHADS21 or CHA2DS2-VASc2 allow a rough estimate of thromboembolic risk and the identification of those patients who may benefit from anticoagulant therapy.
In the last few years, a large number of studies have assessed the possibility of increasing the performance of the aforementioned scores with the addition of analytical parameters3,4 In this regard, renal function has received particular attention. Several investigators have shown that the prevalence of AF is higher in patients with chronic renal disease (CKD) than in the general population.5 On the other hand, renal dysfunction has emerged as a strong predictor of adverse events in patients with AF.6-10 In the ROCKET-AF and ATRIA study cohorts, impaired renal function was shown to be a potent predictor of stroke and systemic embolism in patients with nonvalvular AF at moderate to high risk of stroke. This led the authors into proposing the inclusion of renal function in stroke risk stratification in patients with AF.11
The Cokcroft-Gault, Modification of Diet in Renal Disease (MDRD) and Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI) equations are available for the estimation of glomerular filtration rate (GFR). Some studies have compared the prognostic value of these formulas in the general population,12,13 in individuals at high risk of kidney disease,14 patients admitted for exclusion of myocardial ischemia15 and in subjects with a myocardial infarction16-18 or stroke.19 The MDRD formula has been consistently outperformed by both the Cockcroft-Gault15,17 and the CKD-EPI 12-14,16,19 algorithms in these different clinical contexts. However, to this date no comparison between these equations has been performed in patients with non-valvular atrial fibrillation concerning their ability to predict major adverse cardiac events, stroke or transient ischemic attack (TIA) and all-cause mortality.
To test and compare the prognostic value of the re-expressed 4-variable MDRD, Cockcroft-Gault and CKD-EPI formulae in a cohort of patients with non-valvular AF.
Cross-sectional study of 555 consecutive patients with non-valvular AF undergoing transesophageal echocardiogram at our Echocardiographic Laboratory, enrolled during a 36-month period. Using collected baseline data at the time of admission and outcome data, we tested the prognostic performance of three different formulae for the estimation of GFR (Cokcroft-Gault, re-expressed isotope dilution mass spectrometry [IDMS]-traceable MDRD and CKD-EPI), namely their ability to predict the occurrence of a major cardiac adverse event, ischemic cerebrovascular events (stroke or TIA) and all-cause mortality. Furthermore, the ability of each of the aforementioned equations to add prognostic power to CHADS2 score was also assessed.
Patients and Eligibility Criteria
From October 2008 to September 2011, 613 patients with AF underwent transesophageal echocardiogram at our Echocardiography Laboratory with the purpose of evaluating the appropriateness/safety of electrical cardioversion (576 cases), assessing the severity of suspected or previously known mitral valve disease (19 cases) or as part of routine non-disabling stroke evaluation (28 patients). Forty-eight patients were excluded due to the presence of significant valvular dysfunction (defined as rheumatic valvular disease or the presence of prosthetic heart valves, according to the 2012 focused update of the ESC Guidelines for the management of AF,20 plus any severe valvular stenosis or regurgitation).
All patients were required to have had a creatinine measurement in the previous 24 hours, if admitted at the emergency department, or in the previous 6 months if the transesophageal echocardiogram was programmed and the patient had been clinically stable during that time window. Ten patients did not fulfill laboratory criteria and, therefore, the remaining 555 patients comprised the study sample.
Through extensive review done by 4 co-investigators blind to the purpose of the study, baseline overall group characterization with information on medication, demographic, anthropometric, clinical, laboratory and echocardiographic data were obtained.
Blood samples were collected at admission in all patients admitted at the emergency department. In those whose transesophageal echocardiogram was a programmed one, results from blood samples collected in the 6-month period before the examination (at a previous admission at the emergency department or as routine procedure) were used. The last creatinine measurement before performing transesophageal echocardiogram was used. Creatinine was measured using the CREA VITROS Chemistry Products assay. Values from 4 to 1238 µmol/L could be detected with this assay and normal expected values would be 58-110 µmol/L in males and 46-92 µmol/L in females. Creatinine measurements were calibrated against an isotope dilution mass spectrometry (IDMS) standardized method, which is the currently recommended method. As the calculation of GFR based on creatinine values at the moment of admission would not be an accurate way of estimating the renal function of patients on dialysis, their GFR was arbitrarily estimated as 5 ml/min.
Glomerular filtration rate was estimated using three currently known formulae: Cockcroft-Gault, the re-expressed (IDMS-traceable) MDRD equation and CKD-EPI. As our laboratory calibrated its serum creatinine measurements to IDMS, as currently recommended, the re-expressed version of the MDRD formula was the one used. For each equation, two sets of three categories were defined. The first was based on cutoffs proposed by the National Kidney Foundation (NKF) classification for Chronic Kidney Disease,21 widely used in the literature: GFR<30 ml/min, 30-59 ml/min and ≥60 ml/min. A different set relied on the defined cutoff value from the ATRIA study for increased risk of stroke in AF patients with renal dysfunction (<45 ml/min)7 and the cut-off for normal GFR (≥90 ml/min) according to the NKF classification.21 To facilitate the reading of the manuscript, GFR was expressed as ml/min. However, the reader should be aware that Cockcroft-Gault creatinine clearance values are usually expressed in ml/min, while GFR estimated by the MDRD and CKD-EPI formulae should be expressed as ml/min/1.73m2.
Study End Points and Patient Follow-up
The primary endpoint was all-cause mortality during follow-up. Secondary outcomes were the occurrence of a primary International Classification of Diseases diagnosis of ischaemic stroke or TIA during follow-up, the former confirmed through cerebral computed tomography when deemed necessary by the attending Neurologist, or any major adverse cardiac event (MACE, including non-fatal myocardial infarction or stroke, and mortality due to a cardiovascular cause such as myocardial infarction, stroke or sudden cardiac death). Myocardial infarction was defined according to its Universal Definition,22 while sudden cardiac death included cases of unexpected natural death from a cardiac cause within a short time period (≤1 hour from the onset of symptoms) or, if not witnessed, when the patient was deemed stable 24 hours before.
Patients were followed for 24.0±11.1 months following their discharge. Follow-up data were obtained through review of clinical records from outpatient clinic and hospital ward or emergency department admissions (including invasive or non-invasive examinations, if necessary) and through phone calls by the end of each 6-month period for patients not followed at our institution.
Statistical analysis was done using SPSS, v.17.0. When needed, baseline characteristics are described with mean ± standard deviation for continuous data and counts and proportions for categorical data. The Kolmogorov-Smirnov test was used to test the normal distribution of continuous variables. The Chi-square test, Student’s t-test and non-parametric equivalent tests were used when appropriate. Regression estimation techniques were applied to replace missing values whenever the number of missing values was negligible, otherwise cases with missing values would have been omitted. P values <0.05 (two-sided) were considered statistically significant.
The Cockcroft-Gault, re-expressed MDRD and CKD-EPI formulae were used to estimate the GFR. Subsequently, the three equations were compared through the following methods:
Receiver operating characteristic (ROC) curve analysis - to evaluate the discriminative performance of each formula in the prediction of primary and secondary endpoints; to assess whether models comprising the CHADS2 score and each one of the GFR estimation formulae would outperform CHADS2 score alone in the prediction of the primary endpoint; areas under the curve (AUC) comparisons were performed using MedCalc for Windows version 9.2.0.1;
Chi-square for trend (gamma) - to evaluate the overall tendency of increasing event rates with increasing risk strata using all GFR equations (in both sets of three categories);
Multivariate survival analysis with Cox regression - to assess whether any of the GFR formulae could add prognostic power to the CHADS2 score in the prediction of cerebrovascular ischaemic events;
Integrated discrimination improvement (IDI) and net reclassification improvement (NRI) indexes - to analyze whether any of the three formulae could reclassify a significant proportion of patients into more appropriate risk categories, compared to the others. A comparison was made between the two formulae showing better performance in previous tests.
The NRI was calculated according to the method described by Pencina et al.23 to quantify these reclassifications. A positive NRI translates a net overall successful reclassification of subjects into more appropriate risk categories (e.g. a patient who reaches the primary endpoint that is reclassified into higher risk groups with the new formula), while a negative NRI represents a worse reclassification with the new risk stratification scheme. The amount of overall reclassification is translated by the extent of the NRI (a percent value). The IDI, which may be seen as a continuous form of the NRI, assesses improvement in risk discrimination by estimating the change in the difference in the mean predicted probabilities of the outcome between those with and without the outcome in question.24
Average age was 68.5±10.5, 32.8% (n=182) were female and the majority of patients had Caucasian ethnicity (98.9%; n=549).
Sixty-eight patients (12.3%) reached the primary endpoint, while 30 (5.4%) and 8 (1.5%) were admitted for an ischaemic cerebrovascular event or a myocardial infarction, respectively. Fifty-seven patients (10.3%) had a MACE. Patients reaching the primary endpoint had an average GFR 56.8±28.7 ml/min when estimated by the MDRD formula, 44.8±32.0 ml/min through Cockcroft-Gault and 55.0±26.8 ml/min with the CKD-EPI equation. The average GFR for patients with a MACE was 59.1±26.1 ml/min when estimated by the MDRD formula, 51.1±32.9 ml/min through Cockcroft-Gault and 58.7±26.1 ml/min with CKD-EPI.
Overall characterization of study sample is found on Table 1.
Table 1. Description of Study Sample
| Overall (n=555) |
|---|
| Anthropometric and clinical data |
| Age | 68.46±10.5 |
| Female | 32.8% (182) |
| Body Mass Index | 28.11±5.18 |
| Est.AF episode duration < 1 week | 20.0% (111) |
| Est.AF episode duration >1 month | 34.6% (192) |
| Chronic Dialysis | 1.4% (8) |
| Congestive heart failure | 44.5% (247) |
| Hypertension | 79.8% (443) |
| Diabetes mellitus | 23.2% (129) |
| Previous stroke or TIA | 14.1% (78) |
| Vascular disease * | 49.2% (273) |
| CHADS2 | 1.87±1.16 |
| CHA2DS2VASc | 3.17±1.69 |
| Medication |
| Oral anticoagulants (prior) | 31.9% (177) |
| Oral anticoagulants (post-discharge) | 55.3% (307) |
| Prior ACEi/ARB-II | 69.4% (385) |
| Prior statin | 42.5% (236) |
| Renal function and laboratory data |
| GFR using MDRD | 66.18±25.0 |
| GFR using Cockcroft-Gault | 71.33±35.6 |
| GFR using CKD-EPI | 66.62±24.2 |
| Creatinine (umol/L) | 110.57±87.44 ** |
| Blood urea nytrogen (mmol/L) | 8.94±5.21 |
| Haemoglobin (g/dL) | 13.99±4.27 |
| INR | 1.47±0.75 |
| INR ≥ 2.0 | 20.0% (111) *** |
| Echocardiographic data |
| Left atrium volume (ml/m2) | 58.95±22.86 |
| LVEF < 55% | 24.9% (138) |
| LVEF ≤ 35% | 9.5% (53) |
| LAA thrombus | 10.8% (60) |
| Protuberant aortic plaque | 29.2% (162) |
| Clinical endpoints |
| All-cause mortality | 12.3% (68) |
| Cerebrovascular event | 5.4% (30) |
| Myocardial infarction | 1.5% (8) |
| MACE | 10.3% (57) |
Legend: GFR – glomerular filtration rate; MDRD - Modification of Diet in Renal Disease; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration equation; AF – atrial fibrillation; TIA – transient ischemic attack; ACEi - angiotensin converting enzyme inhibitor; ARB-II - angiotensin II receptor blocker; LVEF – left ventricle ejection fraction; LAA – left atrial appendage; MACE – major adverse cardiac event. * - vascular disease defined as having at least one of the following: myocardial infarction, peripheral artery disease or complex aortic plaque. ** Equivalent to 1.25±0.99 mg/dL *** – 54.8% of those undergoing oral anticoagulation
Distribution of patients according to the previously defined two sets of GFR cutoff values is illustrated on Table 2.
Table 2. Distribution of patients according to the previously defined two sets of GFR cutoff values
| ≥ 60 ml/min | 30-59 ml/min | < 30 ml/min |
|---|
| MDRD | 60.7% (n=337) | 32.1% (n=178) | 7.2% (n=40) |
| Cockcroft-Gault | 60.9% (n=338) | 29.5% (n=164) | 9.6% (n=53) |
| CKD-EPI | 62.1% (n=345) | 30.1% (n=167) | 7.8% (43) |
| ≥ 90 ml/min | 45-89 ml/min | < 45 ml/min |
|---|
| MDRD | 21.4% (n=119) | 63.1% (n=350) | 15.5% (n=86) |
| Cockcroft-Gault | 25.8% (n=143) | 54.4% (n=302) | 19.8% (n=110) |
| CKD-EPI | 18.4% (n=102) | 59.8% (n=332) | 21.8% (n=121) |
Legend: GFR – glomerular filtration rate; MDRD - Modification of Diet in Renal Disease; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration equation.
Comparison Between GFR Estimation Formulae
Through ROC curve analysis, the discriminative performances of the three tested formulae in the prediction of the primary endpoint were assessed:
MDRD AUC 0.624±0.039, 95% CI 0.560-0.672, p<0.001
Cockcroft-Gault AUC 0.749±0.028, 95% CI 0.706-0.787, p<0.001
CKD-EPI AUC 0.641±0.034, 95% CI 0.596-0.685, p<0.001
Comparison of ROC curves revealed that the Cockcroft-Gault equation was significantly superior to both MDRD (difference between areas = 0.125, p<0.001) and CKD-EPI (difference between areas = 0.107, p<0.001) formulae, while CKD-EPI was superior to MDRD (difference between areas = 0.017, p=0.011).
MDRD AUC 0.586±0.054, 95% CI 0.528-0.657, p<0.001
Cockcroft-Gault AUC 0.673±0.049, 95% CI 0.628-0.716, p<0.001
CKD-EPI AUC 0.604±0.054, 95% CI 0.557-0.649, p<0.001
Comparison of ROC curves showed that the Cockcroft-Gault equation was marginally superior to both MDRD (difference between areas = 0.087, p=0.041) and CKD-EPI (difference between areas = 0.069, p=0.063) formulae, while no significant difference was found between CKD-EPI and MDRD (difference between areas = 0.018, p=0.120).
Finally, the AUCs for the prediction a MACE were:
MDRD AUC 0.597±0.041, 95% CI 0.521-0.642, p<0.001
Cockcroft-Gault AUC 0.676±0.036, 95% CI 0.631-0.719, p<0.001
CKD-EPI AUC 0.600±0.040, 95% CI 0.554-0.645, p<0.001
Cockcroft-Gault’s discriminative performance for the prediction of MACE was superior to both MDRD’s (difference between areas = 0.079, p=0.009) and CKD-EPI’s (difference between areas = 0.076, p=0.012) formulae, while CKD-EPI was similar to MDRD (difference between areas = 0.003, p=0.215).
Figure 1-2 illustrate comparisons between the three formulae in the prediction of primary and secondary outcomes.
Figure 1. Comparison between MDRD, Cockcroft-Gault and CKD-EPI in the prediction of all-cause mortality risk
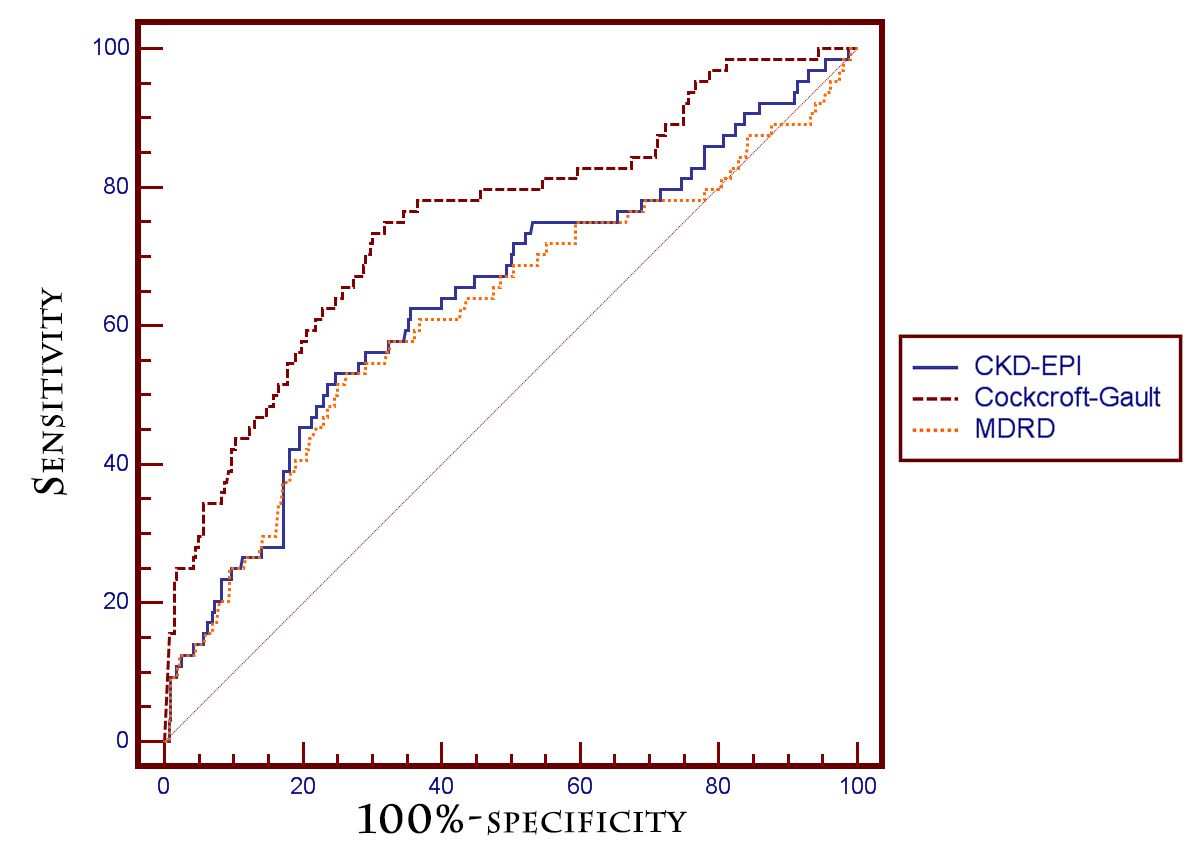
Figure 2. Comparisons between MDRD, Cockcroft-Gault and CKD-EPI in the prediction of ischemic cerebrovascular events (left) and MACE (right)

To evaluate whether the variable “weight” could be the confounder, an additional comparison between the Cockcroft-Gault formula and two new multivariate models including the parameter “weight” and either the MDRD or CKD-EPI equations was performed. Cockcroft-Gault alone was superior to both “CKD-EPI + weight” (difference between areas: 0.028) and “MDRD + weight” (difference between areas: 0.046) in the prediction of the primary endpoint. In the prediction of a cerebrovascular event, Cockcroft-Gault alone was also superior to both “CKD-EPI + weight” (difference between areas: 0.046) and “MDRD + weight” (difference between areas: 0.049).
Chi-Square for Trend (gamma)
The overall tendency of increasing event rates with increasing risk strata were assessed and compared between formulae. Table 3 and Table 4 illustrate the incidence of primary and secondary endpoints according to the previously explained stratification in two sets of three categories each, along with the chi-square for trend (gamma). Gamma for trend was consistently and significantly higher with the Cockcroft-Gault formula for all endpoints. MDRD was similar to CKD-EPI when GFR cut-offs were ≥60 ml/min, 30-59 ml/min and <30 ml/min, but considerably less reliable with the second set of categories (≥90 ml/min, 45-89 ml/min, <45 ml/min).
Table 3. Overall tendency of increasing event rates with increasing risk strata using all GFR equations – Set 1.
| All-cause mortality |
|---|
| GFR (ml/min) | ≥ 60 | 30-59 | < 30 | p | Gamma for trend |
| MDRD | 9.4% | 18.2% | 28.9% | <0.001 | 0.404±0.095 |
| Cockcroft-Gault | 5.7% | 19.7% | 47.7% | < 0.001 | 0.692±0.066 |
| CKD-EPI | 8.9% | 18.4% | 28.9% | <0.001 | 0.429±0.097 |
| Ischaemic cerebrovascular event |
|---|
| GFR (ml/min) | ≥ 60 | 30-59 | < 30 | p | Gamma for trend |
| MDRD | 5.3% | 6.5% | 7.9% | 0.751 | 0.123±0.168 |
| Cockcroft-Gault | 3.2% | 7.3% | 12.6% | 0.009 | 0.467±0.139 |
| CKD-EPI | 5.3% | 6.1% | 7.9% | 0.789 | 0.110±0.178 |
| MACE |
|---|
| GFR (ml/min) | ≥ 60 | 30-59 | <30 | p | Gamma for trend |
| MDRD | 9.6% | 15.3% | 18.4% | 0.083 | 0.262±0.112 |
| Cockcroft-Gault | 6.4% | 14.6% | 27.3% | < 0.001 | 0.497±0.099 |
| CKD-EPI | 8.9% | 12.9% | 18.4% | 0.124 | 0.249±0.123 |
Legend: GFR – glomerular filtration rate; MDRD - Modification of Diet in Renal Disease; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration equation; MACE – Major adverse cardiac event.
Table 4. Overall tendency of increasing event rates with increasing risk strata using all GFR equations – Set 2.
| All-cause mortality |
|---|
| ≥ 90 | 45-89 | <45 | p | Gamma for trend |
| MDRD | 12.2% | 10.2% | 24.6% | 0.001 | 0.309±0.113 |
| Cockcroft-Gault | 6.7% | 9.9% | 34.1% | <0.001 | 0.555±0.094 |
| CKD-EPI | 9.1% | 10.3% | 25.5% | <0.001 | 0.391±0.110 |
| Ischaemic cerebrovascular event |
|---|
| ≥ 90 | 45-89 | <45 | p | Gamma for trend |
| MDRD | 1.2% | 6.3% | 7.9% | 0.124 | 0.333±0.140 |
| Cockcroft-Gault | 1.7% | 4.7% | 12.1% | 0.003 | 0.539±0.136 |
| CKD-EPI | 1.1% | 5.8% | 9.4% | 0.047 | 0.436±0.135 |
| MACE |
|---|
| ≥ 90 | 45-89 | <45 | p | Gamma for trend |
| MDRD | 9.6% | 10.1% | 19.3% | 0.027 | 0.266±0.120 |
| Cockcroft-Gault | 5.8% | 7.9% | 25.3% | <0.001 | 0.493±0.111 |
| CKD-EPI | 8.9% | 8.2% | 19.8% | 0.003 | 0.314±0.127 |
Legend: GFR – glomerular filtration rate; MDRD - Modification of Diet in Renal Disease; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration equation; MACE – Major adverse cardiac event.
Using Cox Regression for survival analysis (forward conditional method), the predictive model for all-cause mortality included the CHADS2 score (p=0.002, HR 1.366, 95% CI 1.125-1.660) and the Cockcroft-Gault formula (p<0.001, HR 0.970, 95% CI 0.961-0.979), excluding the MDRD and CKD-EPI equations.
The predictive model for cerebrovascular event included the Cockcroft-Gault formula (p<0.001, HR 0.971, 95% CI 0.956-0.986), excluding the CHADS2 score and the MDRD and CKD-EPI equations.
Finally, the multivariate model for MACE prediction included both CHADS2 (p=0.016 HR 1.328, 95% CI 1.053-1.673) and the Cockcroft-Gault formula (p<0.001, HR 0.975, 95% CI 0.965-0.985), excluding MDRD and CKD-EPI.
When performing Cox Regression using the CHA2DS2-VASc score instead of CHADS2, the variables included in all predictive models were the same. Likewise, the separate inclusion of all parameters of the CHADS2 score in a Cox Regression analysis for all-cause mortality prediction included variables Diabetes Mellitus (HR 1.97, p=0.009), age > 75 (HR 1.66, p=0.050) and the continuous Cockcroft-Gault equation (HR 0.970, p<0.001), excluding the remaining CHADS2score parameters and GFR estimation formulae. A similar analysis for the prediction of an ischemic cerebrovascular event included the Cockcroft-Gault equation (HR 0.973, p<0.001), excluding all other parameters.
In the prediction of stroke or TIA, a multivariate predictive model including the CHADS2 score and Cockcroft-Gault estimated GFR was superior to a model including both CHADS2 and CKD-EPI calculated GFR (AUC 0.689±0.052, 95% CI 0.587-0.790 vs. AUC 0.638±0.055, 95% CI 0.530-0.746) and to CHADS2 alone (AUC 0.689±0.052, 95% CI 0.587-0.790 vs. AUC 0.591±0.057, 95% CI 0.479-0.703).
Figure 3 illustrates cumulative survival and event-free survival (free of stroke and myocardial infarction), respectively, at mean CHADS2 score (1.97) according to Cockcroft-Gault’s GFR risk stratification.
Figure 3. Cumulative and event-free (free of stroke or myocardial infarction) survival at mean CHADS2 score (1.97) according to Cockcroft-Gault’s glomerular filtration rate risk stratification

Measures of Reclassification
Binary logistic regression was performed including the GFR only, calculated by each of the formula being studied, to obtain estimated probabilities for the occurrence of the primary endpoint. Subsequently, the IDI and relative IDI were calculated to evaluate the improvement in risk stratification with the Cockcroft-Gault formula when compared to CKD-EPI (the two equations with better performances in previous analyses). The IDI and relative IDI for the primary endpoint were 0.092 and 56.4%, respectively, translating a significant and very sizeable improvement in risk stratification. The same analysis for one of the secondary endpoints, MACE, revealed an IDI of 0.037 and a relative IDI of 31.4%.
Category-based NRI provided a different statistical approach to assess the improvement in reclassification by using Cockcroft-Gault instead of CKD-EPI. The former reclassified 24.3% of cases into risk strata that were more accurate representations of observed all-cause mortality risk (p-value 2-sided=0.00045). Moreover, regarding stroke/AIT and MACE, the Cockcroft-Gault formula reclassified 20.4% (p-value 2-sided=0.033) and 15.0% (p-value 2-sided=0.037) of patients into more appropriate risk categories, respectively. Cross-tabulation between Cockcroft-Gault and CKD-EPI is seen on Table 5.
Table 5. Cross-tabulation between the Cockcroft-Gault and CKD-EPI equations
| All-cause mortality | Cockcroft-Gault (GFR in ml/min) |
|---|
| | | ≥ 60 | 30-59 | <30 | |
| Events (n=68) | CKD-EPI (GFR in ml/min) | ≥ 60 | 16 | 6 | 5 | |
| 30-59 | 1 | 21 | 7 | NRI = 24.3% p = 0.00045 |
| <30 | 0 | 2 | 10 | |
| Non-Events (n=487) | ≥ 60 | 298 | 20 | 2 | |
| 30-59 | 28 | 104 | 3 | |
| < 30 | 0 | 8 | 24 | |
| Cerebrovascular events | Cockcroft-Gault (GFR in ml/min) |
|---|
| | | ≥ 60 | 30-59 | <30 | |
| Events (n=30) | CKD-EPI (GFR in ml/min) | ≥ 60 | 11 | 3 | 1 | |
| 30-59 | 0 | 8 | 3 | NRI = 20.4% p = 0.033 |
| <30 | 0 | 1 | 3 | |
| Non-Events (n=525) | ≥ 60 | 299 | 23 | 6 | |
| 30-59 | 29 | 120 | 7 | |
| <30 | 0 | 9 | 32 | |
| MACE | Cockcroft-Gault (GFR in ml/min) |
|---|
| Cockcroft-Gault (GFR in ml/min) | | | | | | |
| | | ≥ 60 | 30-59 | <30 | |
| Events (n=57) | CKD-EPI (GFR in ml/min) | | | | | |
| ≥ 60 | 19 | 5 | 3 | NRI = 15.0% p = 0.037 |
| 30-59 | 2 | 15 | 4 | |
| <30 | 0 | 2 | 7 | |
| Non-Events (n=498) | ≥60 | 298 | 20 | 4 | |
| 30-59 | 27 | 108 | 6 | |
| | <30 | 0 | 8 | 27 | |
Legend: GFR – glomerular filtration rate; CKD-EPI – Chronic Kidney Disease Epidemiology Collaboration equation; MACE – Major adverse cardiac event; NRI – Net reclassification improvement index.
In our cohort of patients with non-valvular AF undergoing transesophageal echocardiogram, the Cockcroft-Gault formula was significantly more accurate than both the re-expressed 4-variable MDRD and CKD-EPI equations in predicting the risk of all-cause mortality, ischemic cerebrovascular events or MACE during an average follow-up of two years. Through ROC curve analysis, multivariate analysis and measures of reclassification, we have shown that the categorization of kidney function using the Cockcroft-Gault equation more appropriately stratifies AF patients according to risk of hard clinical endpoints. In fact, sizeable proportions of patients were reclassified into more appropriate risk categories with the use of Cockcroft-Gault instead of CKD-EPI. The re-expressed MDRD formula seemed the least accurate in predicting the risk of primary and secondary endpoints.
There has not been consensus regarding which formula should be used for the estimation of GFR in AF patients. MDRD was the only formula used in the Chronic Renal Insufficiency Cohort (CRIC), which evaluated the prevalence of AF in patients with less advanced chronic kidney disease;5 in the ATRIA study;7 by Kastarinen H et al., who evaluated the potential association between GFR and carotid intima-media thickness in middle-aged adults;9 by Guo Y et al. in their study of the potential relationship between renal dysfunction and increased risk of stroke and death in female patients with AF;25 and by Roldan V and colleagues in a study that evaluated the effect of renal function on prognosis in anticoagulated patients with AF and assessed the changes in renal function during a long-term follow-up.26 On the other hand, the CKD-EPI equation was the formula of choice in a study by Providência R et al10 and, along with Cockcroft-Gault (but without establishing a comparison) in a post-hoc analysis of the ARISTOTLE trial.4 An investigation by Piccini JP et al. used the Cockcroft-Gault for the validation of the R2CHADS2 Index in the ROCKET AF and ATRIA cohorts.11 In a sub-analysis of PLATO atrial, CKD-EPI exhibited the largest predictive value of all renal markers (including GFR estimated by the Cockcroft-Gault and MDRD equations), with a small additive predictive value of cystatin C.27
Comparisons between CKD-EPI and MDRD in other clinical settings invariably favored the former,12-14,16,19,28 while Cockcroft-Gault was also consistently shown to be superior to MDRD.13,15 However, although comparisons between two formulae have already been performed by different investigators in different clinical contexts, our study is the first to assess and compare the three equations in a cohort of patients with non-valvular AF.
Clinical guidelines recommend that clinical laboratories should report GFR using the MDRD equation whenever serum creatinine measurement was made.20 False-positive CKD due to underestimation of GFR by the MDRD equation is still a concern, but the original CKD-EPI might be able to reduce the false-positive rate.10 In our cohort, CKD-EPI classified a slightly lower percentage of patients as having a GFR<60 ml/min, which apparently corroborates the findings of Matsushita K et al.10 Patients who were reclassified into higher GFR categories using CKD-EPI were in fact less likely to reach one of the primary or secondary endpoints. Certain reasons have been appointed as possible explanations for the apparent superiority of CKD-EPI when compared to MDRD. The former uses a spline for serum creatinine level, which enables better identification of the differing relationships between creatinine level and GFR throughout the range of measured GFRs, and uses a linear instead of a logarithmic term for age.29
Weight, a parameter included in the Cockcroft-Gault GFR estimation, is a prognostic marker per se, as overall frailty is more likely in underweight individuals and these patients are at higher risk for bleeding events. As hemorrhagic risk is also progressively higher with decreasing GFR, and bleeding is a strong predictor of both mortality and thromboembolic events, it is possible that renal dysfunction and low weight act synergistically to increase all-cause mortality in patients with non-valvular AF. To evaluate whether the variable “weight” could be the confounder, additional analyses were performed, demonstrating that, while weight may account for a percentage of the net superiority of the Cockcroft-Gault formula, it does not explain it to its full extent. Additional differences in the coefficients included in the GFR equations may have contributed to the apparent advantage of the Cockcroft-Gault formula.
However, it should not be forgotten that the relationship between all-cause mortality and body mass index has been shown to be U-shaped in several populations,30-32 a phenomenon particularly prominent in the elderly33-35 and those with chronic kidney failure.36 This might affect the interpretation of our results.
Although some studies have not confirmed the independent role of renal dysfunction in the prognostication of patients with AF,37 the overall net evidence is supportive of the inclusion of renal function parameters in the risk stratification of these patients. Our study reinforces this notion. Moreover, the potential validation of our findings in larger studies may eventually shift the focus of attention away from the MDRD formula and encourage the use of CKD-EPI and especially Cockcroft-Gault. Standardization of GFR equation throughout studies may add robustness to future recommendations. Nevertheless, the fact that the Cockcroft-Gault formula has not been re-expressed in order to be used with newer methods of determination of serum creatinine may limit its diagnostic accuracy and should also be considered. Future studies with larger cohorts of patients with AF may allow more definite conclusions.
Limitations of this study
The main limitation of this study concerns the fact that our cohort may not be representative of a general population of AF patients, as we included patients with non-valvular AF undergoing transesophageal echocardiogram, mostly for evaluating the appropriateness of electrical cardioversion. Persistent AF was therefore the most frequently observed, rather than paroxysmal or permanent, but these two represent a large percentage of AF patients. Accurate validation of our results in larger cohorts of non-selected AF patients is warranted.
The use of only one serum creatinine measurement prevents verification of the acute vs. chronic nature of CKD in some of our patients.
As some of the patients who died during follow-up were not autopsied, the exact cause of death was sometimes hard to ascertain. Review of clinical records provided accurate information in those followed at our institution or admitted at the emergency department, but information acquired through phone calls is usually of lower quality.
The search for a validated assessment method to estimate the GFR in elderly patients is a topic of ongoing research and it remains unknown which formula serves this purpose better. While the CDK-EPI formula38 and the Berlin Initiative equation39 have shown potential applicability in this context, to our knowledge the Cockcroft-Gault formula has never been unequivocally validated as a reliable method to estimate GFR in older subjects. Even so, a 2010 systematic review suggested that, although there is insufficient evidence, the Cockcroft-Gault formula may still be valuable in evaluating renal function in the elderly.40 In our study sample, the Cockcroft-Gault formula was still the most accurate in predicting mortality in patients ≥75 years old: AUC Cockcroft-Gault 0.689±0.056 vs. AUC MDRD 0.653±0.053 vs. AUC CKD-EPI 0.656±0.053), although differences were not as impressive as in the whole cohort.
It should also be emphasized that a direct measurement of renal function has not been performed and, therefore, we do not know whether the better performance of the Cockcroft-Gault formula was due to the fact that it more accurately assesses renal function or rather that it has a superior ability to capture the overall risk of adverse outcomes regardless of its accuracy in the assessment of the renal function.
The lack of cystatin C data is also a limitation of this study, particularly in the light of recent studies suggesting the best way to estimate GFR is to include both creatinine and cystatin C.39,41 However, cystatin C values were not systematically collected in our patients, therefore this potentially valuable analysis could not be performed.
This study suggests that, in patients with non-valvular AF submitted to transesophageal echocardiogram, the Cockcroft-Gault more appropriately classifies individuals with respect to risk of all-cause mortality, ischaemic cerebrovascular event and major adverse cardiac event. Whether this apparent improvement in risk stratification will translate into improved patient outcomes remains to be determined. The potential validation of our results in larger cohorts of patients may eventually shift the balance in favor of the Cockcroft-Gault or eventually the CKD-EPI equations and away from the MDRD formula.






